

Young-onset colorectal cancer
- PMID: 37105987
- PMCID: PMC10589420
- DOI: 10.1038/s41572-023-00432-7
Young-onset colorectal cancer
Abstract
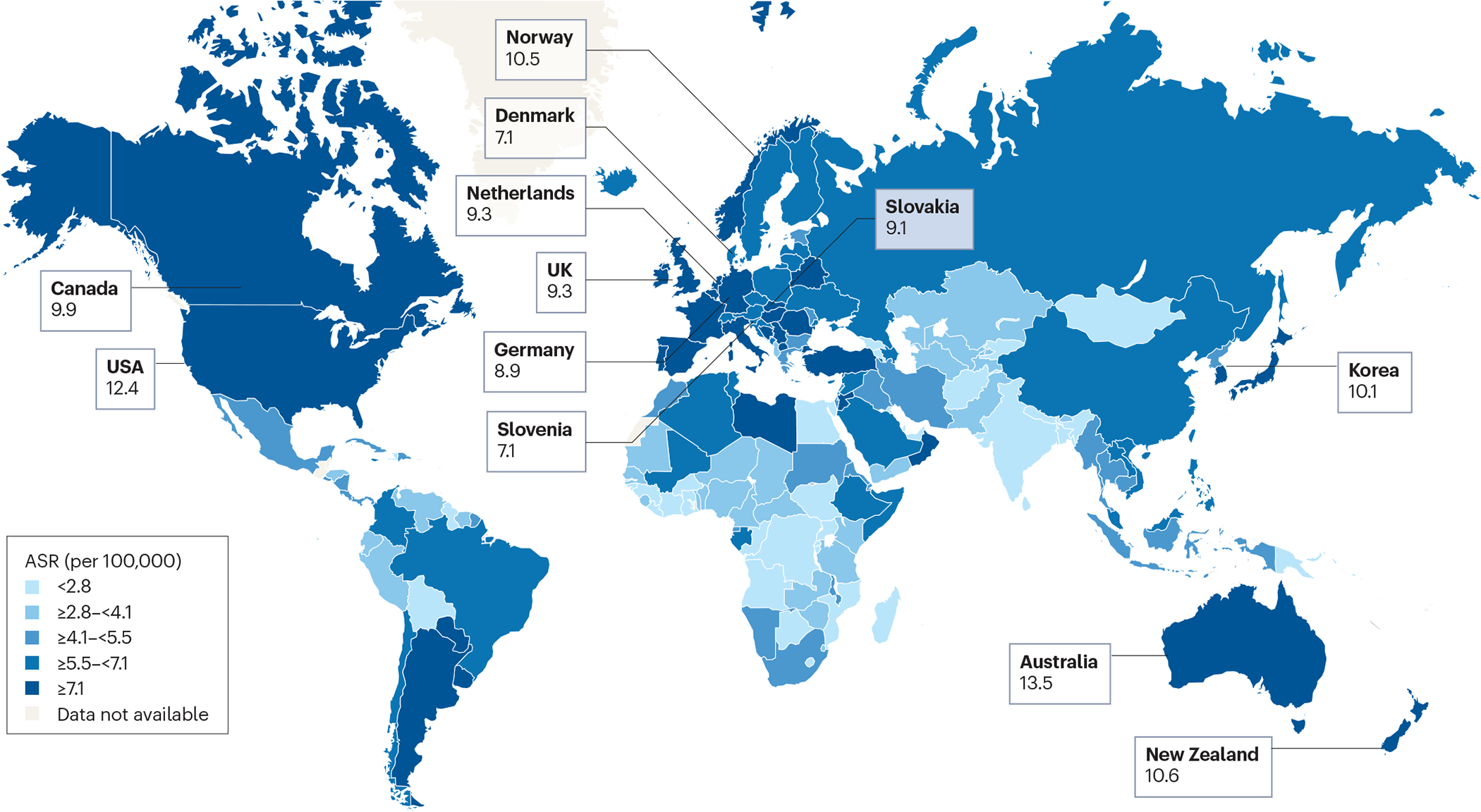
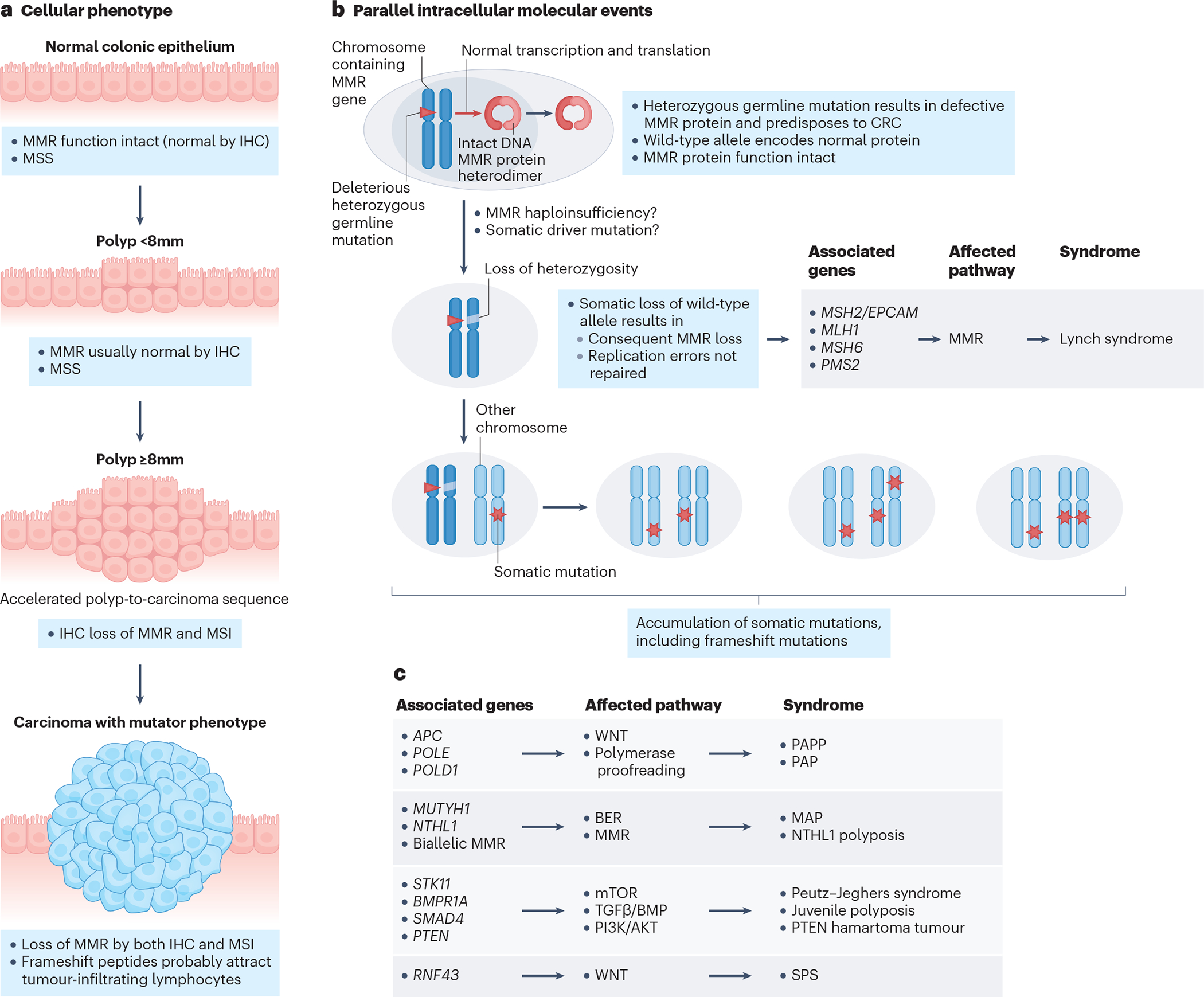
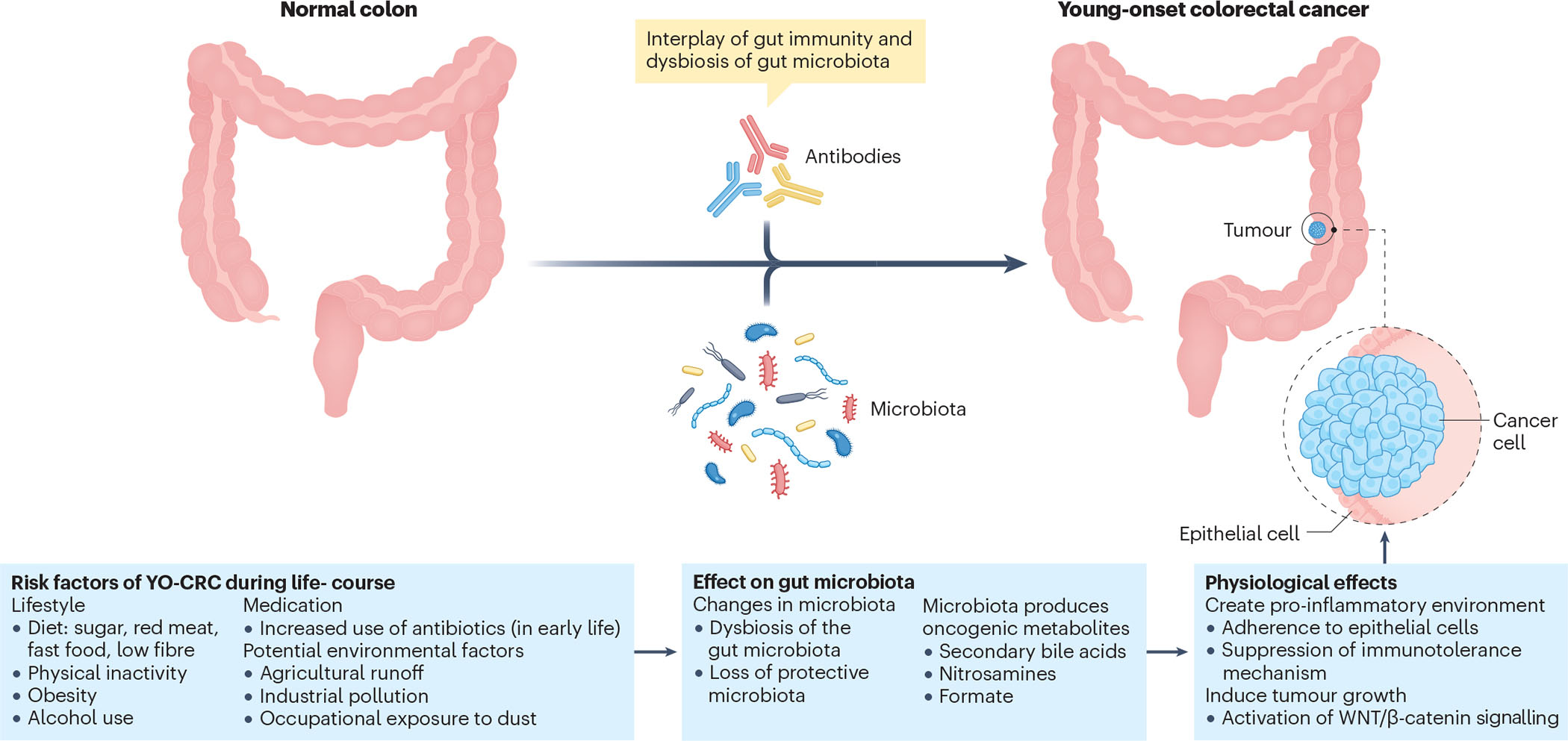
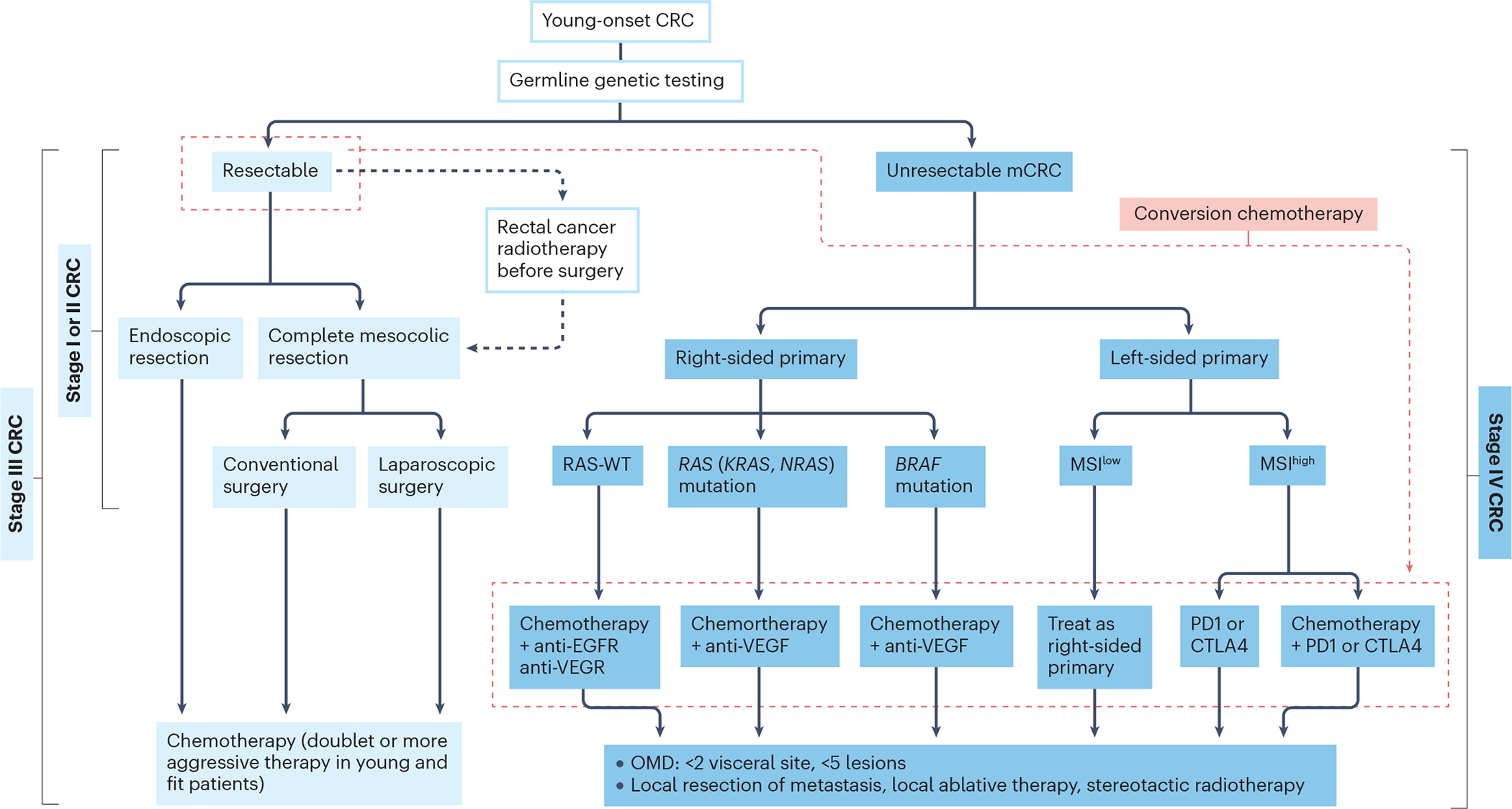
In the past decades the incidence of colorectal cancer (CRC) in people under the age of 50 years has increased, which is referred to as early-onset CRC or young-onset CRC (YO-CRC). YO-CRC is expected to account for 11% of colon cancers and 23% of rectal cancers by 2030. This trend is observed in different parts of the world and in both men and women. In 20% of patients with YO-CRC, a hereditary cancer syndrome is found as the underlying cause; however, in the majority of patients no genetic predisposition is present. Beginning in the 1950s, major changes in lifestyle such as antibiotic use, low physical activity and obesity have affected the gut microbiome and may be an important factor in YO-CRC development. Owing to a lack of screening, patients with YO-CRC are often diagnosed with advanced-stage disease. Long-term treatment-related complications should be taken into account in these younger patients, making the more traditional sequential approaches of drug therapy not always the most appropriate option. To better understand the underlying mechanism and define relationships between environmental factors and YO-CRC development, long-term prospective studies are needed with lifestyle data collected from childhood.
© 2023. Springer Nature Limited.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Siegel RL, Miller KD, and Jemal A, Cancer statistics, 2018. CA Cancer J Clin, 2018. 68(1): p. 7–30. - PubMed
-
- Arnold M, et al. , Global patterns and trends in colorectal cancer incidence and mortality. Gut, 2017. 66(4): p. 683–691. - PubMed
-
- Malvezzi M, et al. , European cancer mortality predictions for the year 2018 with focus on colorectal cancer. Ann Oncol, 2018. 29(4): p. 1016–1022. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
