

CanScreen5, a global repository for breast, cervical and colorectal cancer screening programs
- PMID: 37106168
- PMCID: PMC10202799
- DOI: 10.1038/s41591-023-02315-6
CanScreen5, a global repository for breast, cervical and colorectal cancer screening programs
Abstract
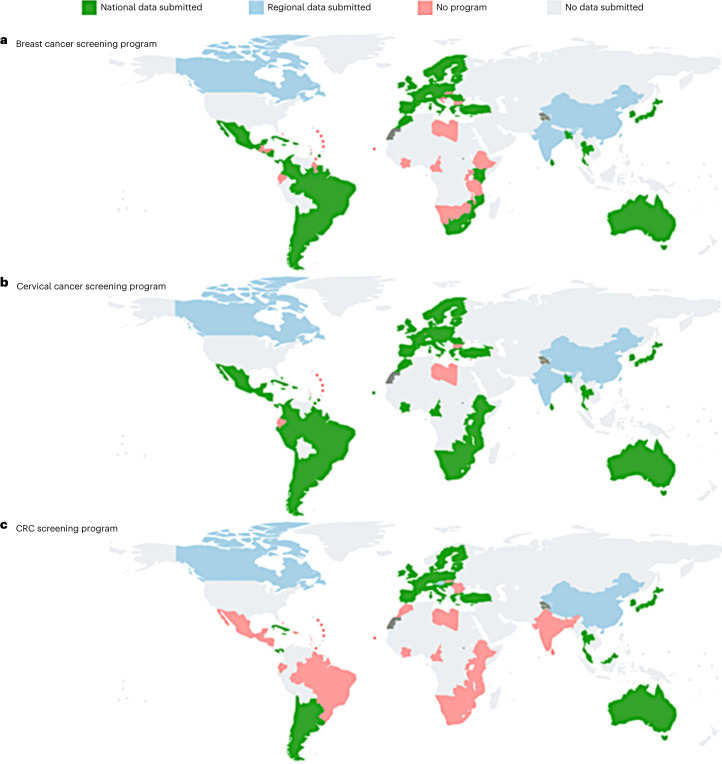
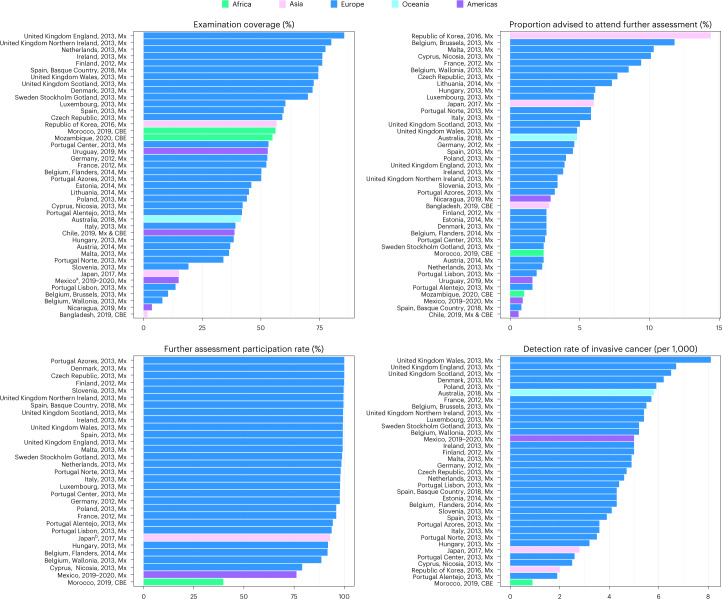
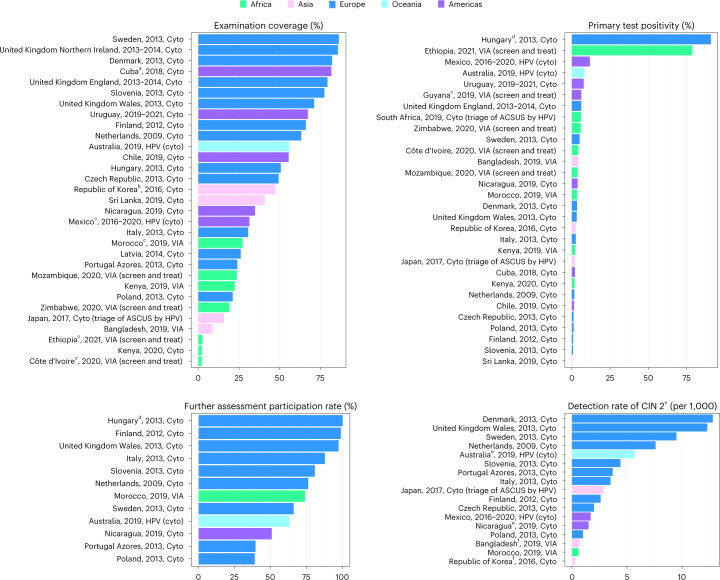
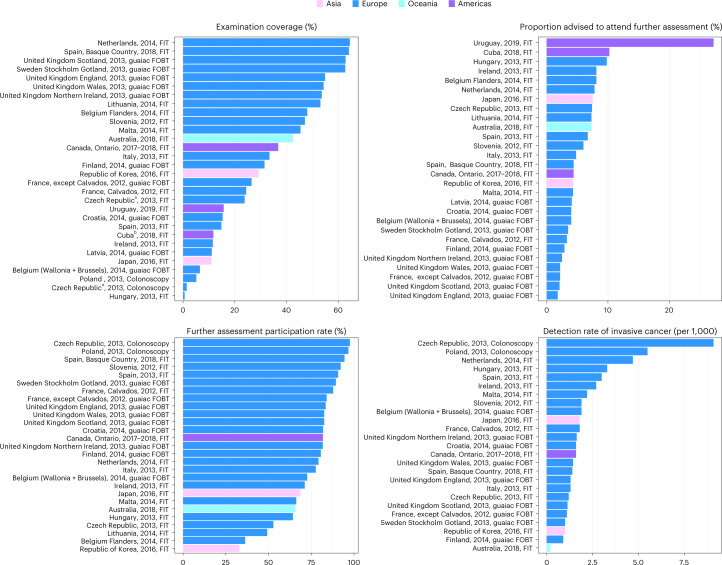
The CanScreen5 project is a global cancer screening data repository that aims to report the status and performance of breast, cervical and colorectal cancer screening programs using a harmonized set of criteria and indicators. Data collected mainly from the Ministry of Health in each country underwent quality validation and ultimately became publicly available through a Web-based portal. Until September 2022, 84 participating countries reported data for breast (n = 57), cervical (n = 75) or colorectal (n = 51) cancer screening programs in the repository. Substantial heterogeneity was observed regarding program organization and performance. Reported screening coverage ranged from 1.7% (Bangladesh) to 85.5% (England, United Kingdom) for breast cancer, from 2.1% (Côte d'Ivoire) to 86.3% (Sweden) for cervical cancer, and from 0.6% (Hungary) to 64.5% (the Netherlands) for colorectal cancer screening programs. Large variability was observed regarding compliance to further assessment of screening programs and detection rates reported for precancers and cancers. A concern is lack of data to estimate performance indicators across the screening continuum. This underscores the need for programs to incorporate quality assurance protocols supported by robust information systems. Program organization requires improvement in resource-limited settings, where screening is likely to be resource-stratified and tailored to country-specific situations.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
A call to improve the quality of screening programs.Nat Med. 2023 May;29(5):1062-1063. doi: 10.1038/s41591-023-02305-8. Nat Med. 2023. PMID: 37106169 No abstract available.
References
-
- World Health Organization. Cancer—Screening and Early Detectionhttps://www.who.int/europe/news-room/fact-sheets/item/cancer-screening-a... (WHO, 2010).
-
- Romero, Y. et al. National cancer control plans: a global analysis. Lancet Oncol.19, e546–e555 (2018). - PubMed
-
- Mandal, R. & Basu, P. Cancer screening and early diagnosis in low- and middle-income countries: current situation and future perspectives. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz61, 1505–1512 (2018). - PubMed
-
- Arbyn, M. et al. European Guidelines for Quality Assurance in Cervical Cancer Screening 2nd edn (Office for Official Publications of the European Communities, 2008).
