

The First Survival Score for Patients Treated with Whole-Brain Radiotherapy Plus Simultaneous Integrated Boost for Brain Metastases
- PMID: 37106785
- PMCID: PMC10135994
- DOI: 10.3390/biology12040585
The First Survival Score for Patients Treated with Whole-Brain Radiotherapy Plus Simultaneous Integrated Boost for Brain Metastases
Abstract
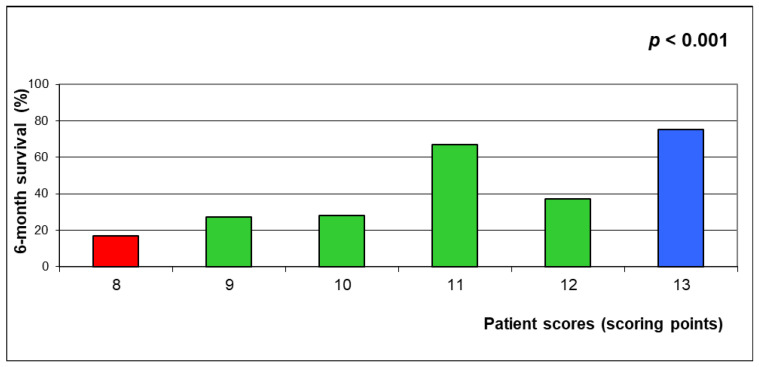
A modern approach for brain metastases includes whole-brain radiotherapy plus simultaneous boost (WBRT+SIB). We developed a survival score in 128 patients treated with WBRT+SIB. Three models, each including three prognostic groups, were created. Positive predictive values (PPVs) for death ≤6 and survival ≥6 months were calculated. On multivariate analyses, performance score (KPS) and the number of brain metastases were significantly associated with survival. On univariate analyses, age showed a strong trend, and extra-cerebral cranial metastases a trend. In Model 1 (KPS, number of lesions), compared groups had 6-month survival rates of 15%, 38% and 57%. In Model 2 (KPS, lesions, age), rates were 17%, 33% and 75%, and in Model 3 (KPS, lesions, age, extra-cerebral metastases), 14%, 34% and 78%. PPVs for death ≤6 and survival ≥6 months were 85% and 57% (Model 1), 83% and 75% (Model 2), and 86% and 78% (Model 3). Thus, all models were accurate in predicting death ≤ 6 months; poor-prognosis patients may not benefit from SIB. Models 2 and 3 were superior in predicting survival ≥ 6 months. Given that Model 3 requires more data (including extensive staging), Model 2 is considered favorable for many patients. If extra-cerebral metastases are already known or extensive staging has been performed, Model 3 can also be used.
Keywords: cerebral metastases; predictive model; simultaneous integrated boost; survival; whole-brain radiotherapy.
Conflict of interest statement
The authors declare no conflict of interest related to this study.
Figures






References
-
- Gondi V., Bauman G., Bradfield L., Burri S.H., Cabrera A.R., Cunningham D.A., Eaton B.R., Hattangadi-Gluth J.A., Kim M.M., Kotecha R., et al. Radiation therapy for brain metastases: An ASTRO clinical practice guideline. Pract. Radiat. Oncol. 2022;12:265–282. doi: 10.1016/j.prro.2022.02.003. - DOI - PubMed
-
- Tsao M.N., Rades D., Wirth A., Lo S.S., Danielson B.L., Gaspar L.E., Sperduto P.W., Vogelbaum M.A., Radawski J.D., Wang J.Z., et al. Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation Oncology evidence-based guideline. Pract. Radiat. Oncol. 2012;2:210–225. doi: 10.1016/j.prro.2011.12.004. - DOI - PMC - PubMed
-
- Andrews D.W., Scott C.B., Sperduto P.W., Flanders A.E., Gaspar L.E., Schell M.C., Werner-Wasik M., Demas W., Ryu J., Bahary J.P., et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase III results of the RTOG 9508 randomised trial. Lancet. 2004;363:1665–1672. doi: 10.1016/S0140-6736(04)16250-8. - DOI - PubMed
-
- Rades D., Janssen S., Dziggel L., Blanck O., Bajrovic A., Veninga T., Schild S.E. A matched-pair study comparing whole-brain irradiation alone to radiosurgery or fractionated stereotactic radiotherapy alone in patients irradiated for up to three brain metastases. BMC Cancer. 2017;17:30. doi: 10.1186/s12885-016-2989-3. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
