

Patients with Chronic Spinal Cord Injury and a Long Period of Evolution Exhibit an Altered Cytokine Production by CD4 and CD8 T Cell Populations
- PMID: 37108209
- PMCID: PMC10138939
- DOI: 10.3390/ijms24087048
Patients with Chronic Spinal Cord Injury and a Long Period of Evolution Exhibit an Altered Cytokine Production by CD4 and CD8 T Cell Populations
Abstract
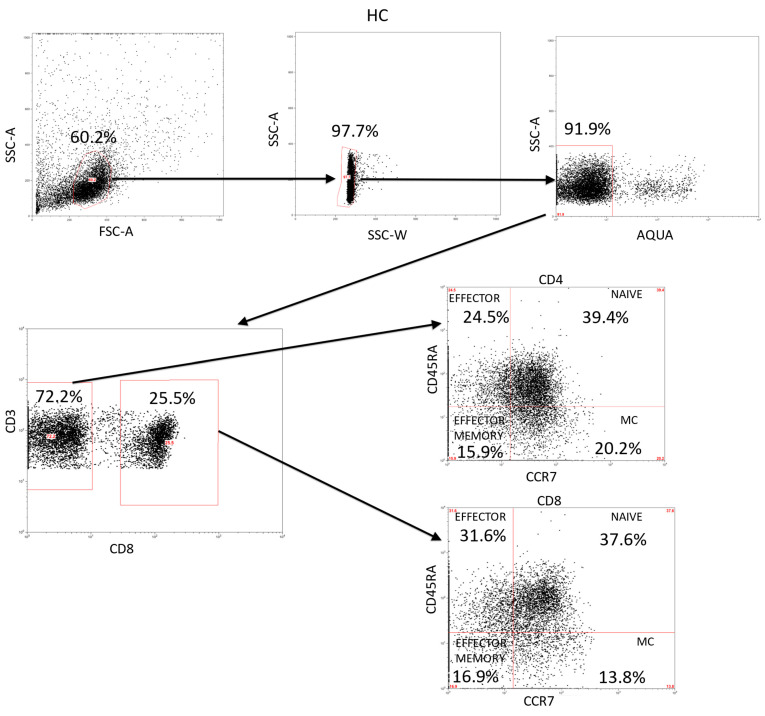
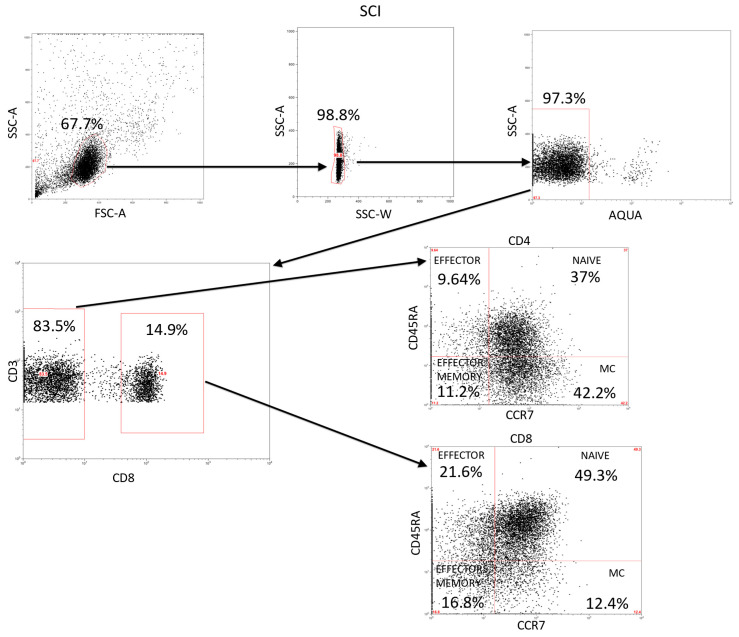
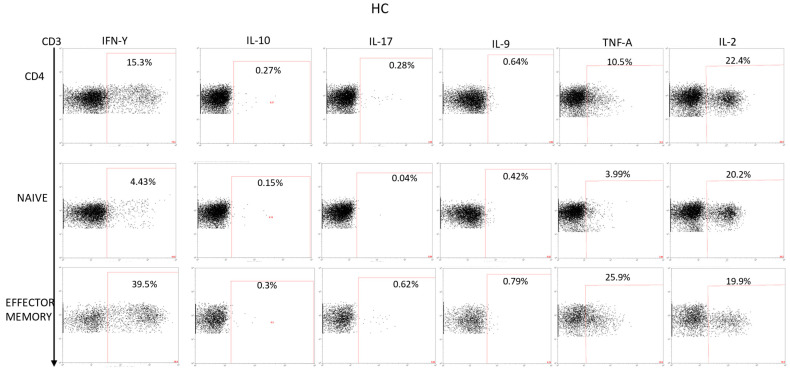
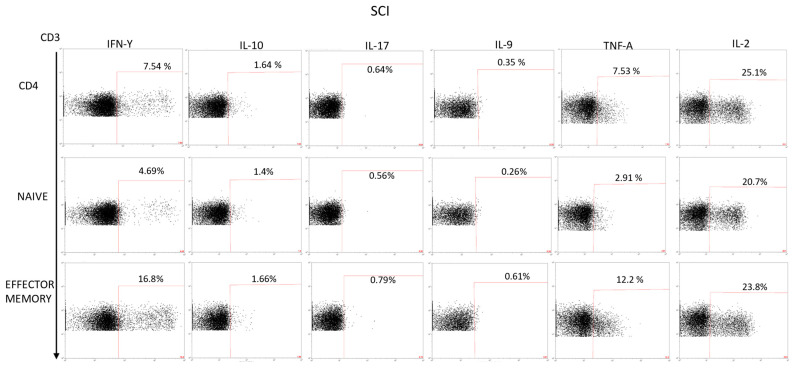
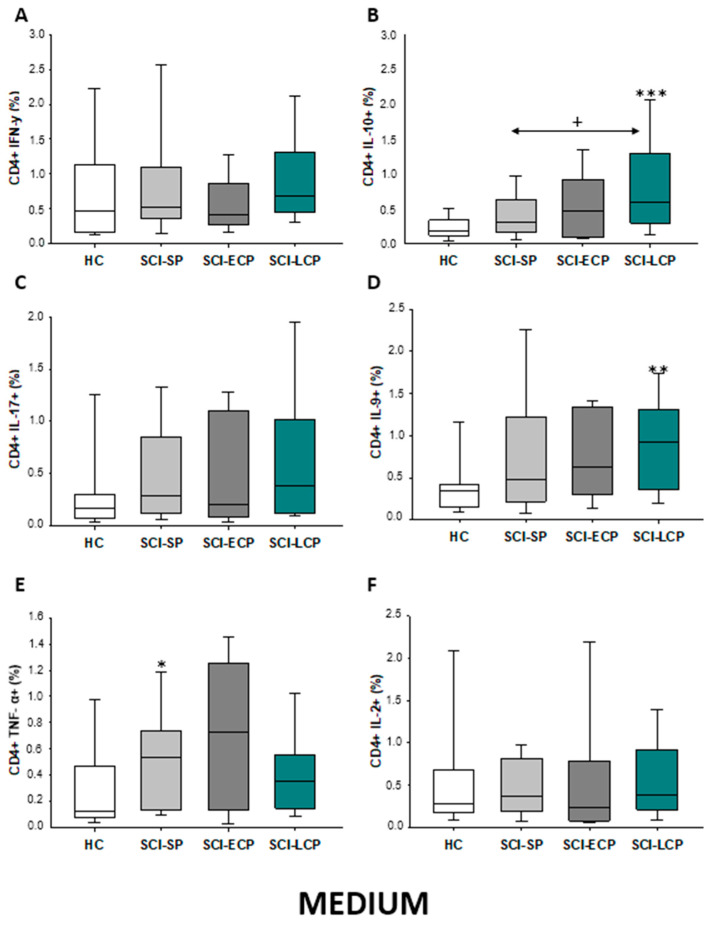
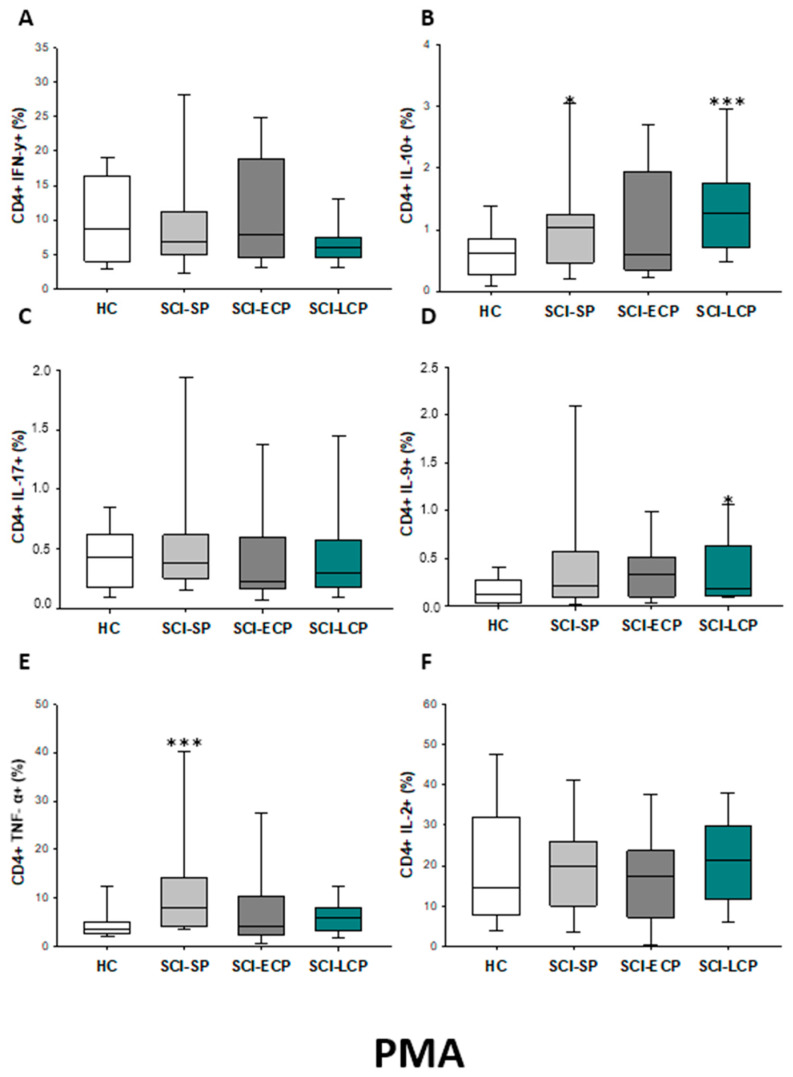
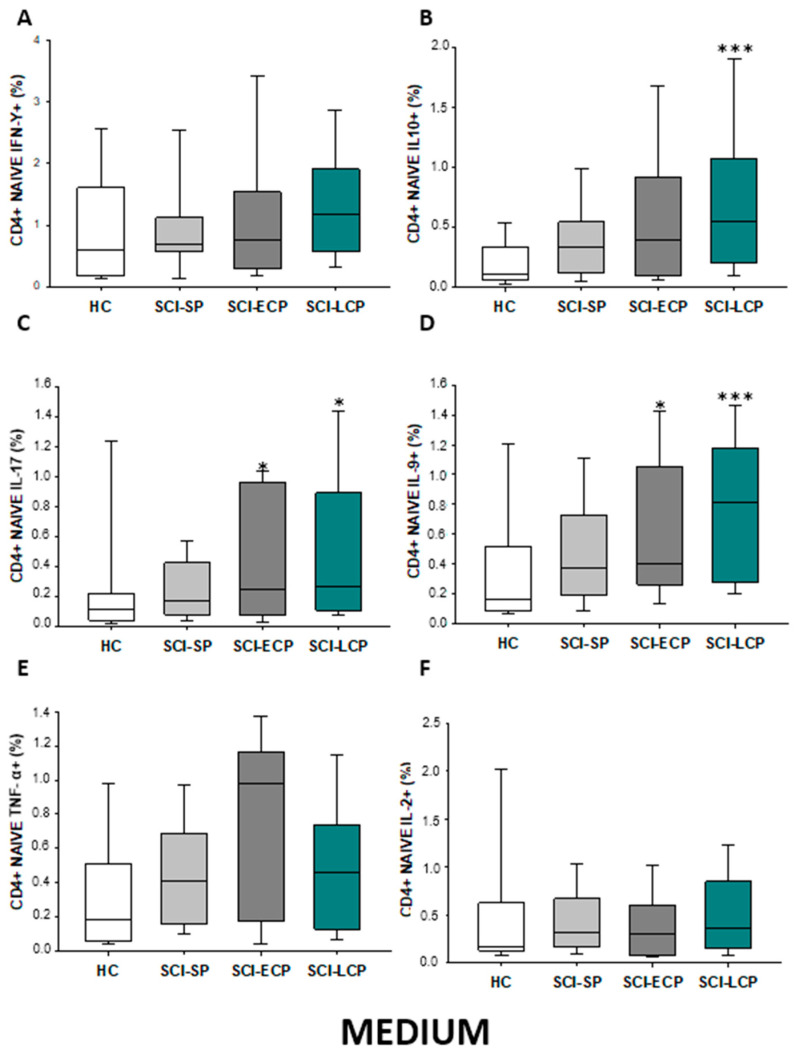
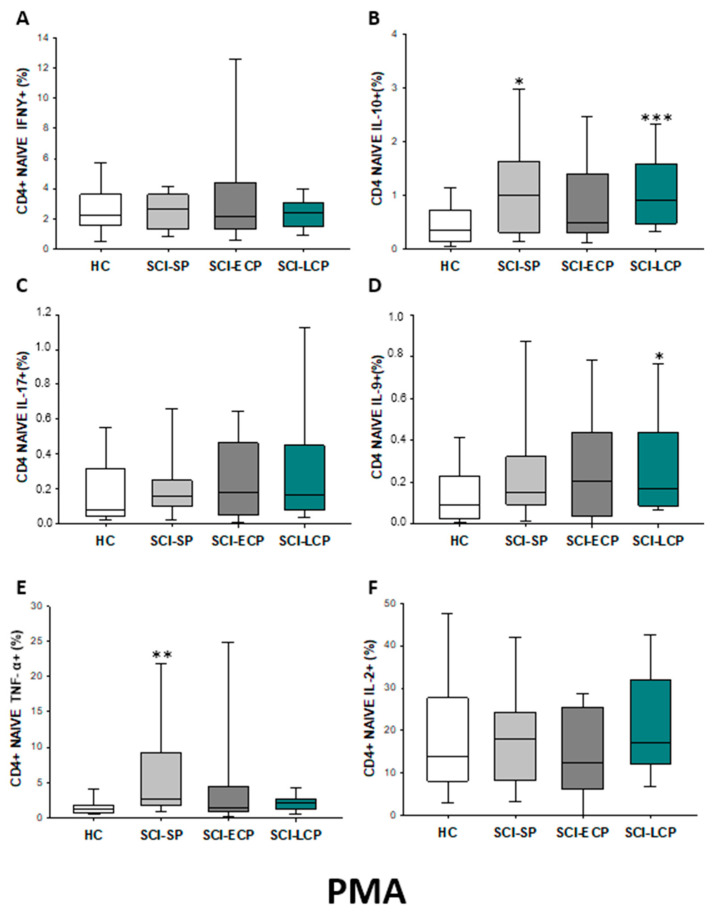
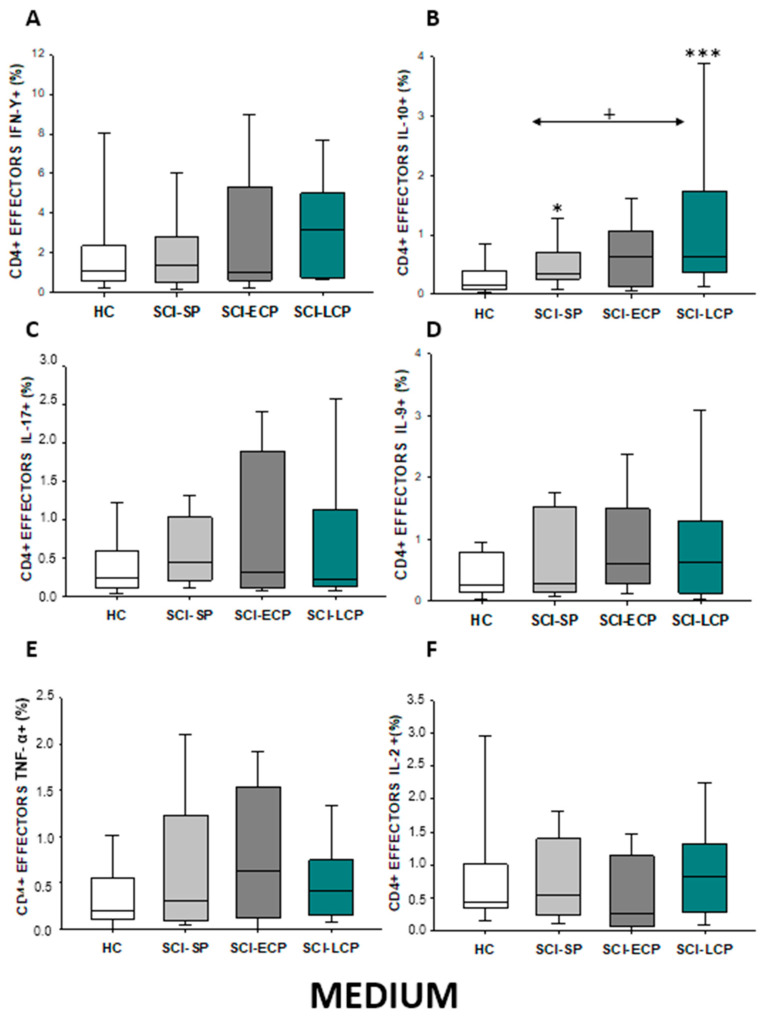
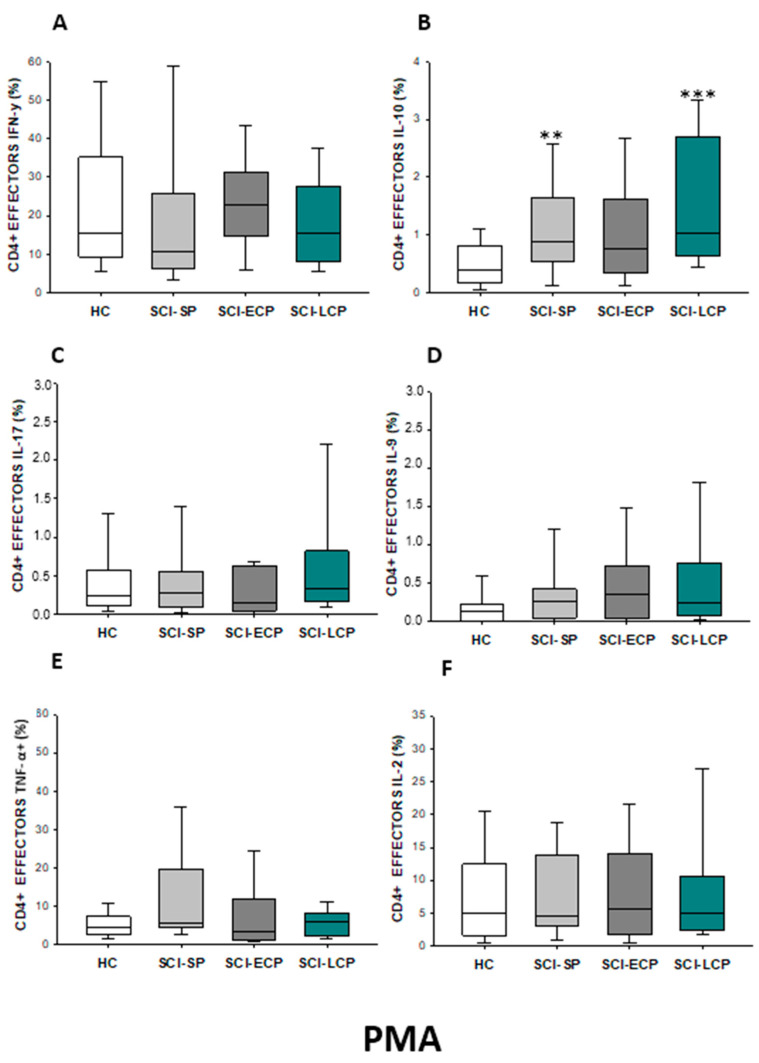
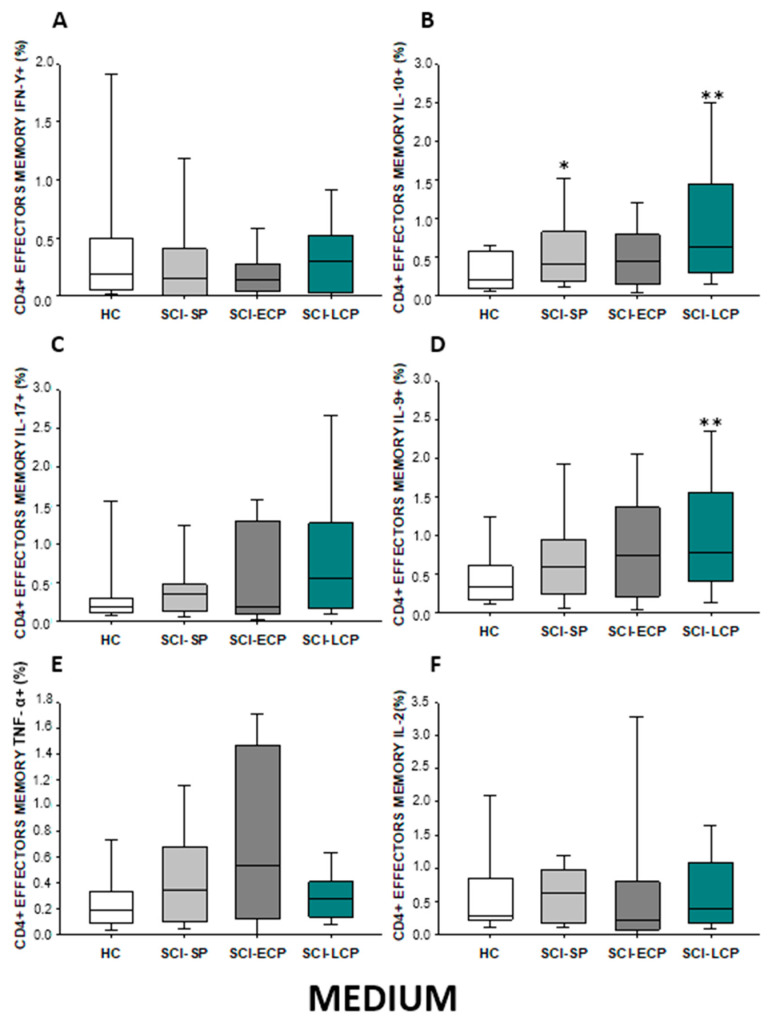
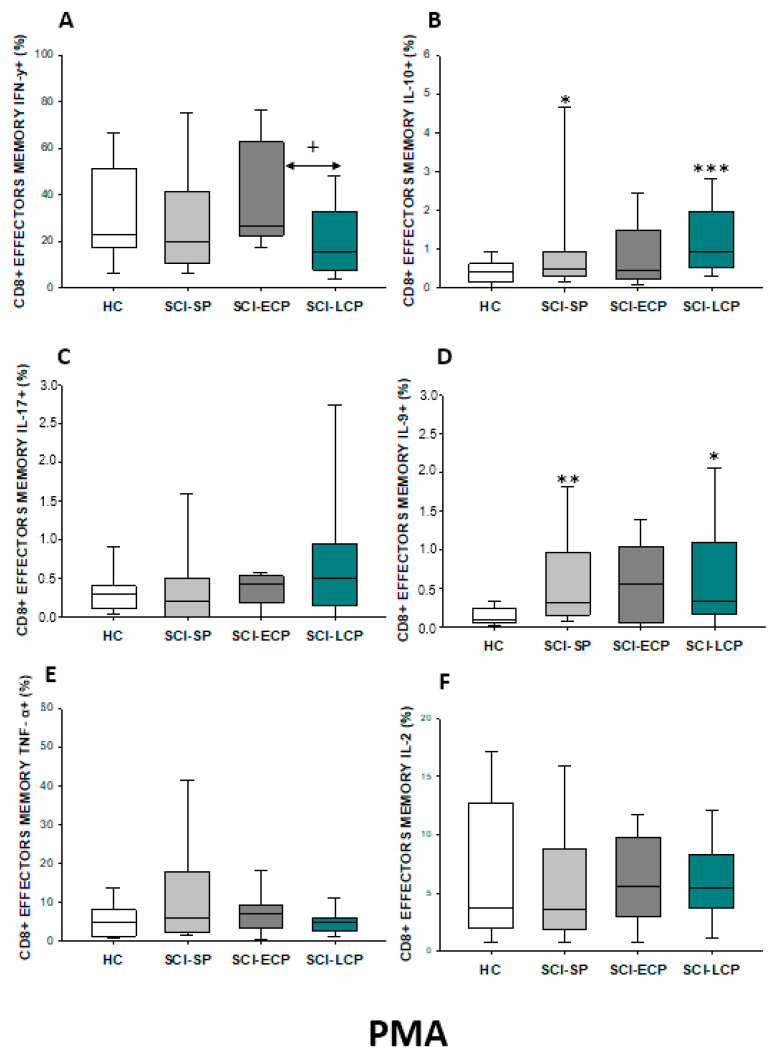
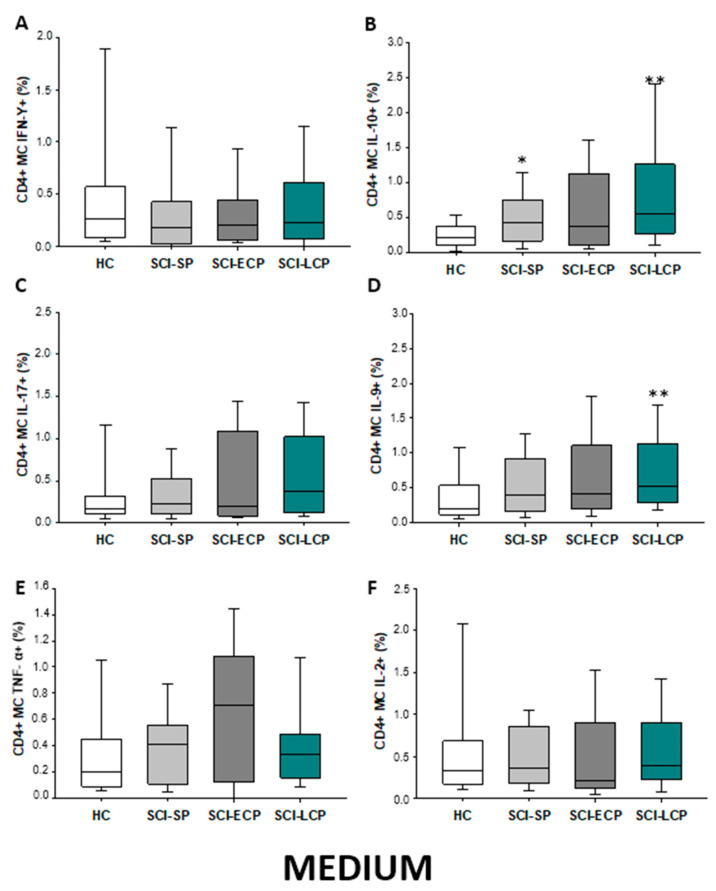
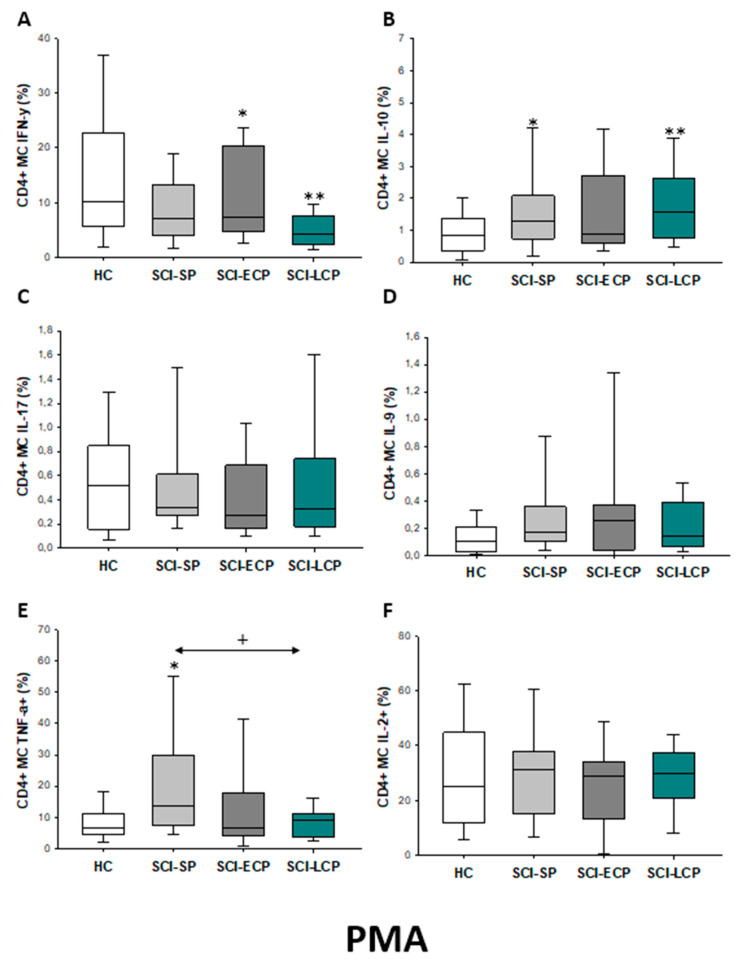
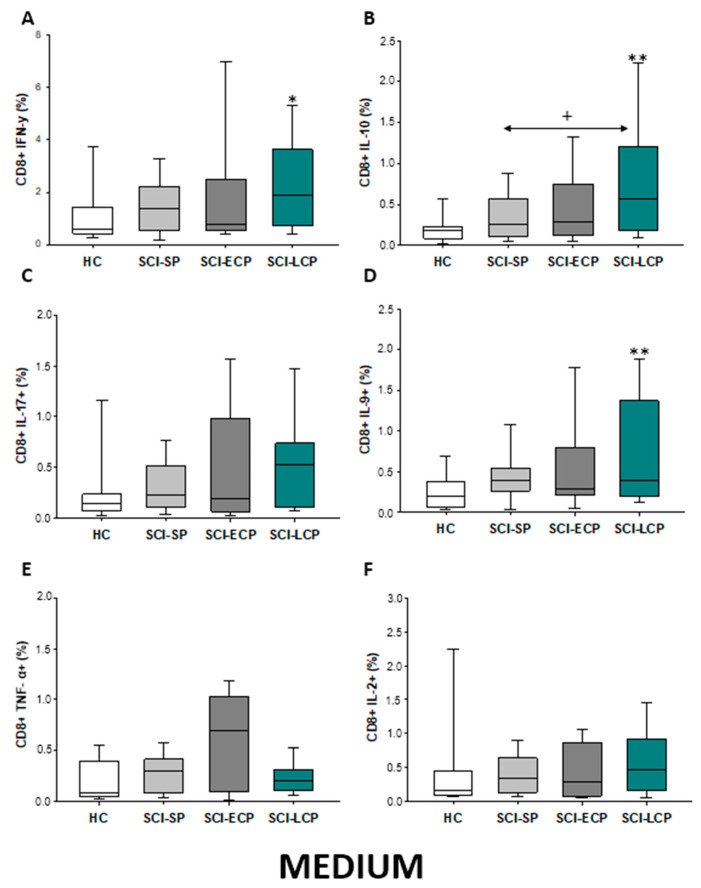
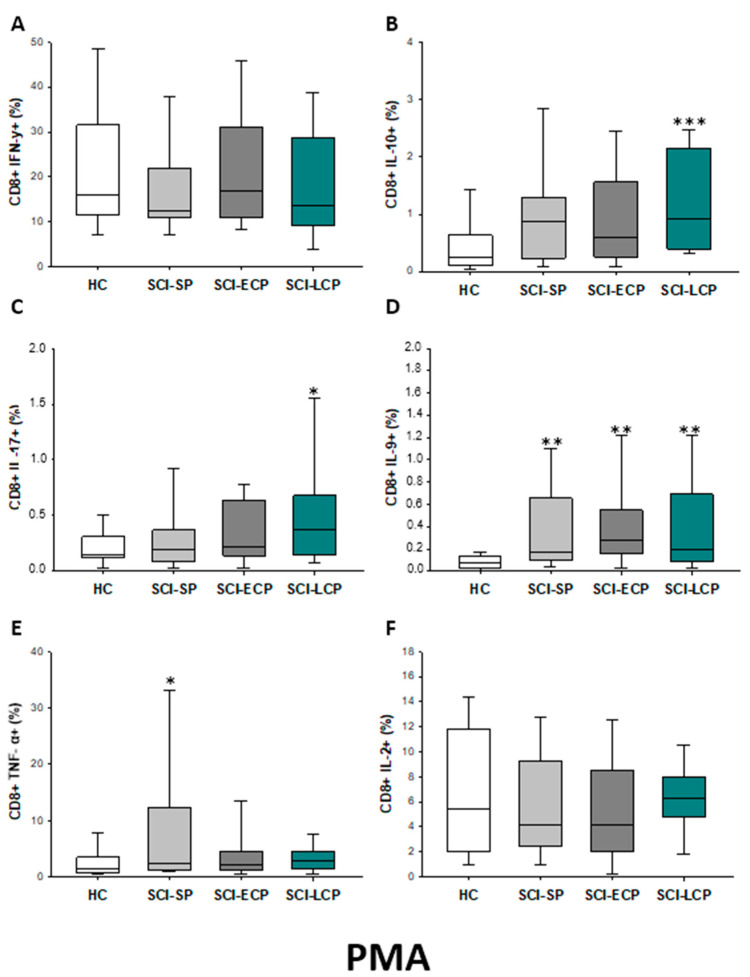
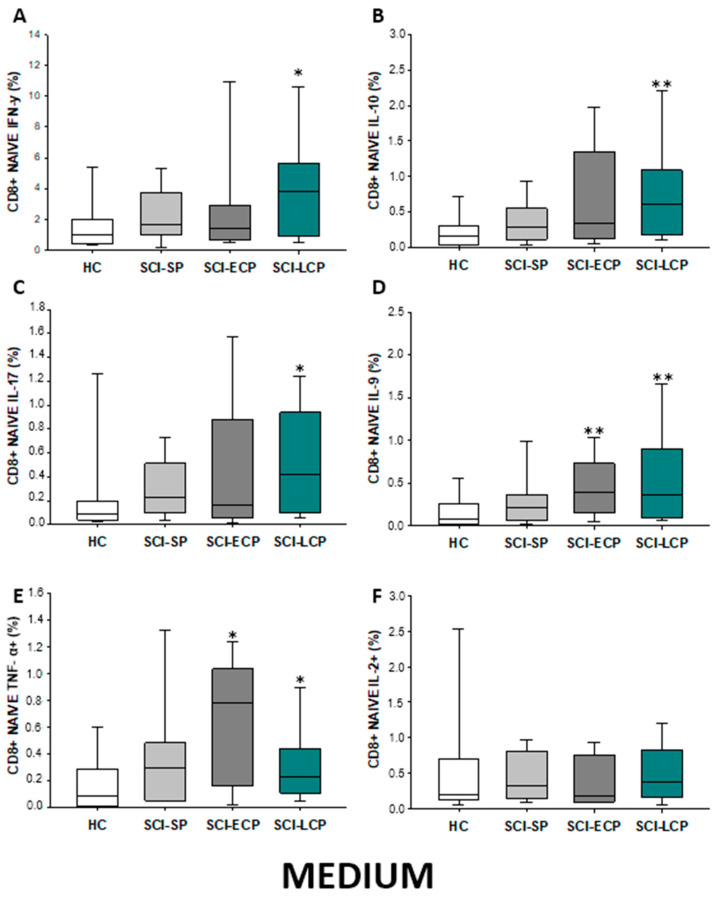
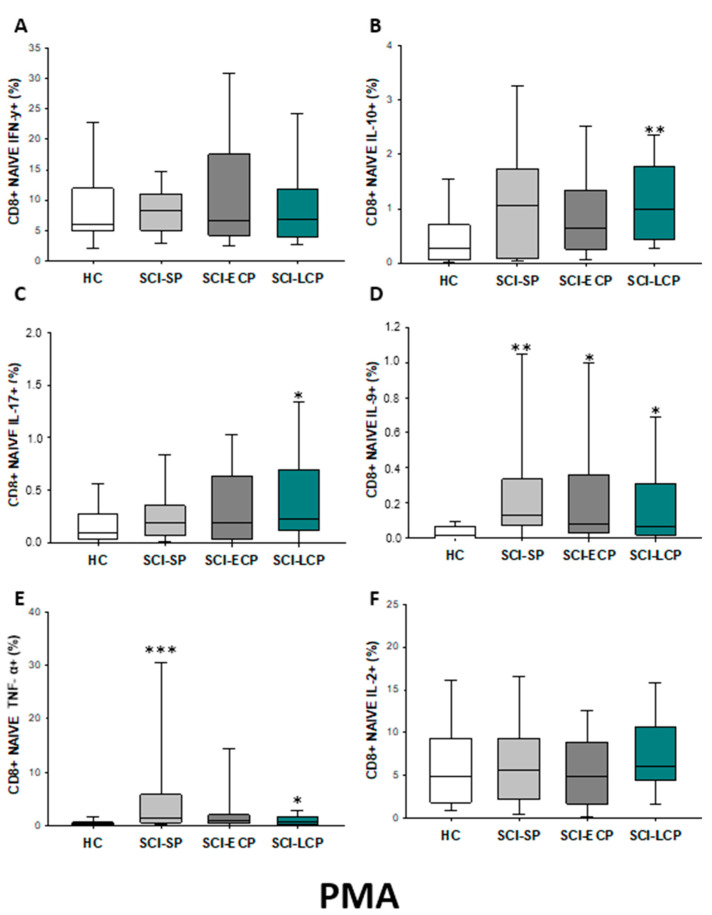
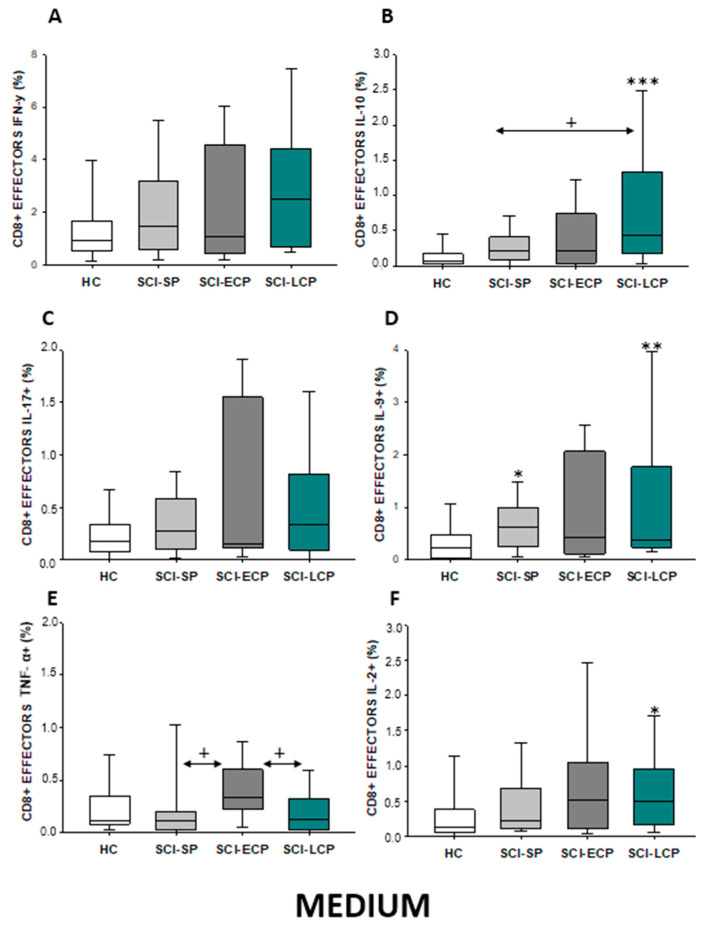
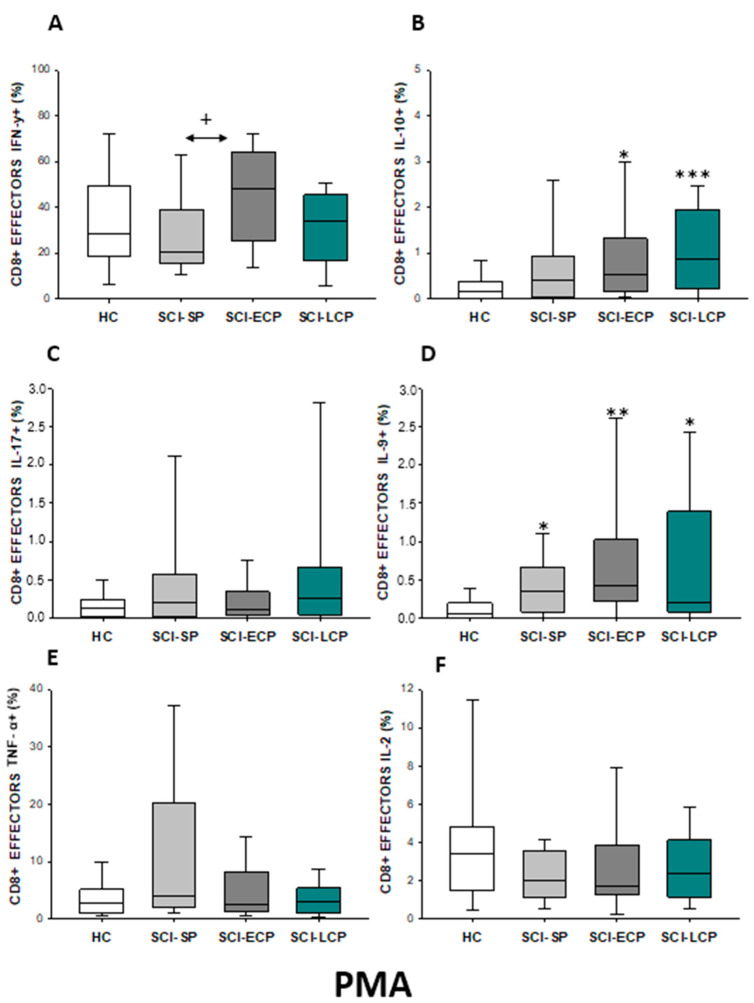
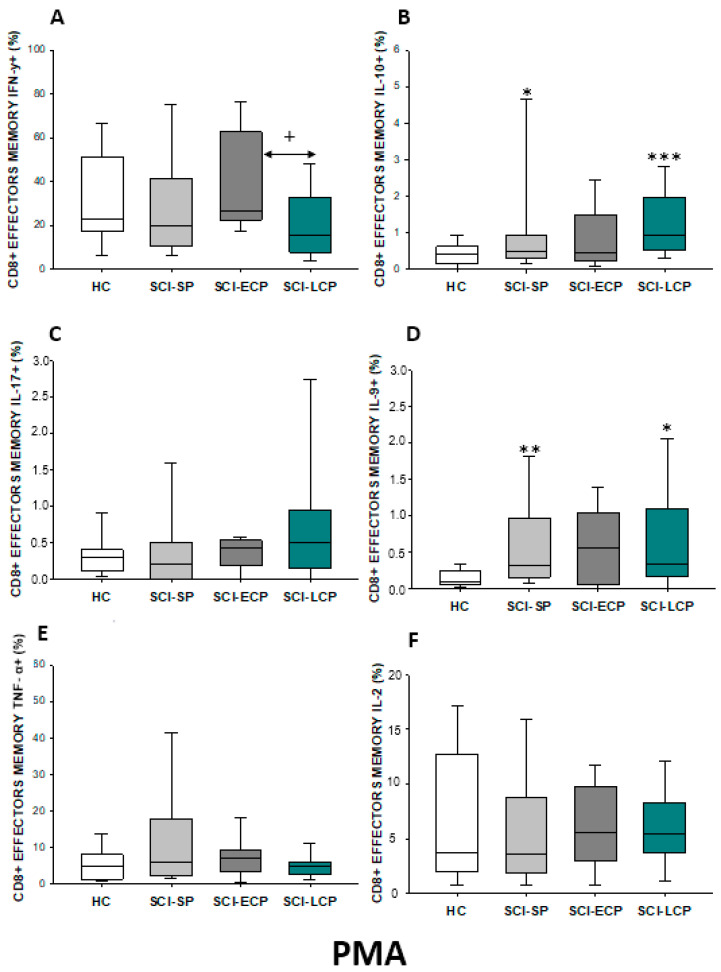
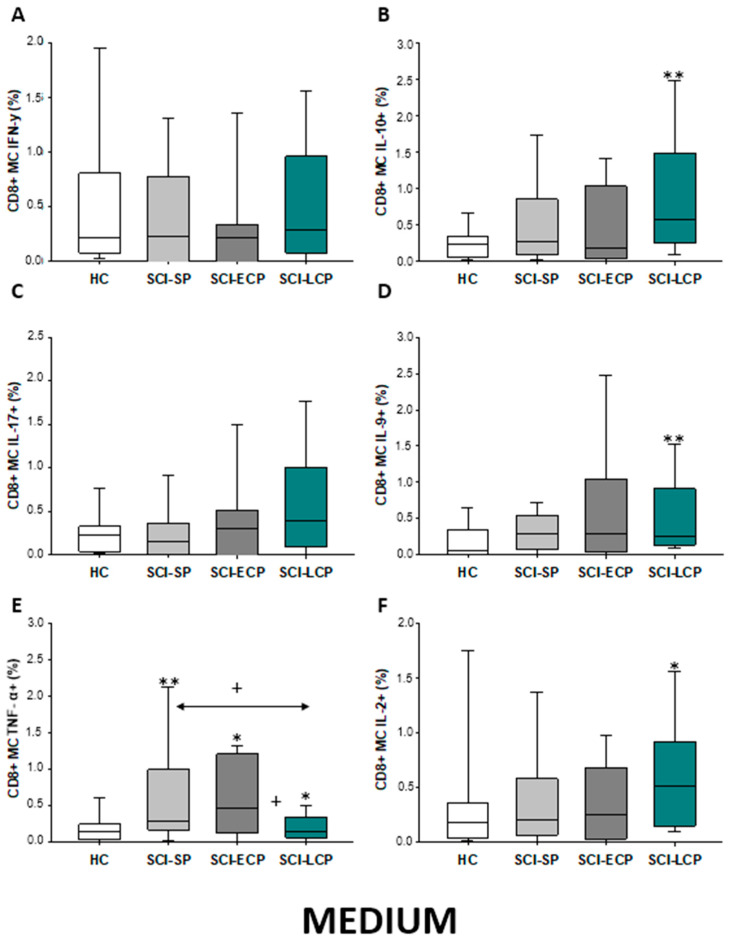
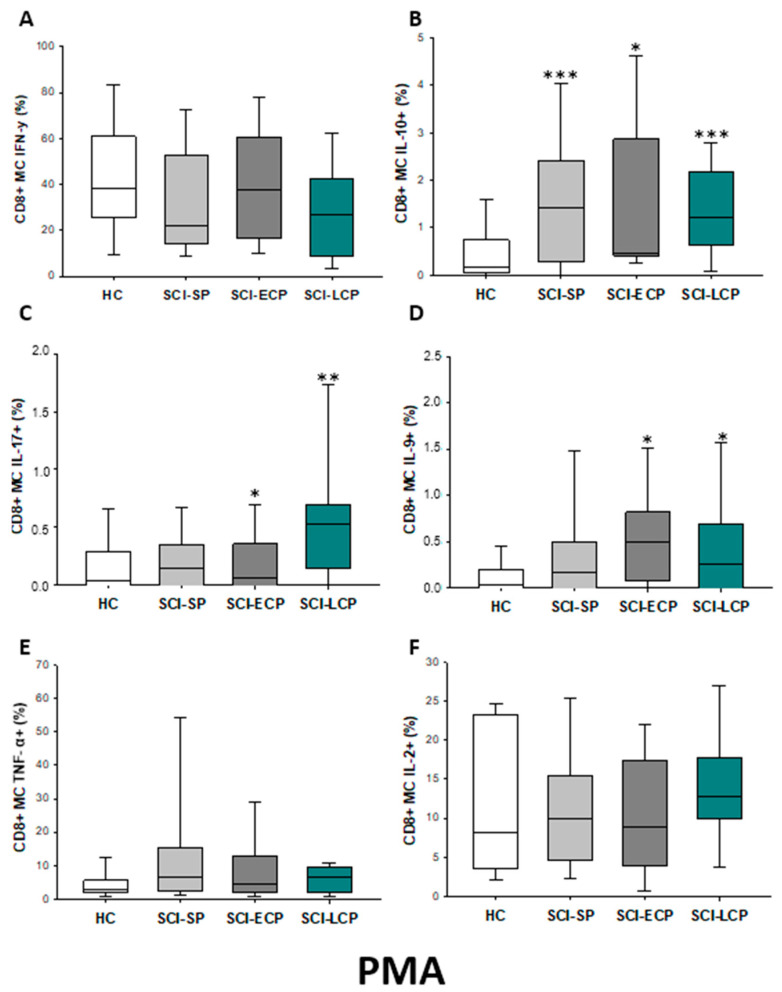
Spinal cord injury (SCI) is a disabling neurological condition coursing with serious multisystem affections and morbidities. Changes in immune cell compartments have been consistently reported in previous works, representing a critical point of study for understanding the pathophysiology and progression of SCI from acute to chronic stages. Some relevant variations in circulating T cells have been noticed in patients with chronic SCI, although the number, distribution, and function of these populations remain to be fully elucidated. Likewise, the characterization of specific T cell subpopulations and their related cytokine production can aid in understanding the immunopathological role of T cells in SCI progression. In this sense, the objective of the present study was to analyze and quantify the total number of different cytokine-producers T cells in the serum of patients with chronic SCI (n = 105) in comparison to healthy controls (n = 38) by polychromatic flow cytometry. Having this goal, we studied CD4 and CD8 lymphocytes as well as naïve, effector, and effector/central memory subpopulations. SCI patients were classified according to the duration of the lesion in chronic SCI with a short period of evolution (SCI-SP) (comprised between 1 and 5 years since initial injury), early chronic phase (SCI-ECP) (between 5 and 15 years since initial injury) and late-chronic phase (SCI-LCP) (>15 years since initial injury). Our results show that patients with chronic SCI exhibited an altered immune profile of cytokine-producer T cells, including CD4/CD8 naïve, effector, and memory subpopulations in comparison to HC. In particular, IL-10 and IL-9 production seems to be importantly altered, especially in patients with SCI-LCP, whereas changes in IL-17, TNF-α, and IFN-γ T cell populations have also been reported in this and other chronic SCI groups. In conclusion, our study demonstrates an altered profile of cytokine-producer T cells in patients with chronic SCI, with marked changes throughout the course of the disease. In more detail, we have observed significant variations in cytokine production by circulating naive, effector, and effector/central memory CD4 and CD8 T cells. Future studies should be directed to explore the possible clinical consequences of these changes or develop additional translational approaches in these groups of patients.
Keywords: T lymphocytes; chronic spinal cord injury (SCI); interleukin 10 (IL-10); interleukin 9.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
A comprehensive look at the psychoneuroimmunoendocrinology of spinal cord injury and its progression: mechanisms and clinical opportunities.Mil Med Res. 2023 Jun 9;10(1):26. doi: 10.1186/s40779-023-00461-z. Mil Med Res. 2023. PMID: 37291666 Free PMC article. Review.
-
Patients with Chronic Spinal Cord Injury Display a Progressive Alteration over the Years of the Activation Stages of the T Lymphocyte Compartment.Int J Mol Sci. 2023 Dec 18;24(24):17596. doi: 10.3390/ijms242417596. Int J Mol Sci. 2023. PMID: 38139422 Free PMC article.
-
Abnormal Characterization and Distribution of Circulating Regulatory T Cells in Patients with Chronic Spinal Cord Injury According to the Period of Evolution.Biology (Basel). 2023 Apr 19;12(4):617. doi: 10.3390/biology12040617. Biology (Basel). 2023. PMID: 37106817 Free PMC article.
-
Effect of human bone marrow mesenchymal stromal cells on cytokine production by peripheral blood naive, memory, and effector T cells.Stem Cell Res Ther. 2015 Jan 5;6(1):3. doi: 10.1186/scrt537. Stem Cell Res Ther. 2015. PMID: 25559824 Free PMC article.
-
Functional Signatures of Human CD4 and CD8 T Cell Responses to Mycobacterium tuberculosis.Front Immunol. 2014 Apr 22;5:180. doi: 10.3389/fimmu.2014.00180. eCollection 2014. Front Immunol. 2014. PMID: 24795723 Free PMC article. Review.
Cited by
-
Effects of altered glycolysis levels on CD8+ T cell activation and function.Cell Death Dis. 2023 Jul 8;14(7):407. doi: 10.1038/s41419-023-05937-3. Cell Death Dis. 2023. PMID: 37422501 Free PMC article. Review.
-
A comprehensive look at the psychoneuroimmunoendocrinology of spinal cord injury and its progression: mechanisms and clinical opportunities.Mil Med Res. 2023 Jun 9;10(1):26. doi: 10.1186/s40779-023-00461-z. Mil Med Res. 2023. PMID: 37291666 Free PMC article. Review.
-
Exploration of biomarkers associated with histone lactylation modification in spinal cord injury.Front Genet. 2025 Jul 2;16:1609439. doi: 10.3389/fgene.2025.1609439. eCollection 2025. Front Genet. 2025. PMID: 40672388 Free PMC article.
-
Patients with Chronic Spinal Cord Injury Display a Progressive Alteration over the Years of the Activation Stages of the T Lymphocyte Compartment.Int J Mol Sci. 2023 Dec 18;24(24):17596. doi: 10.3390/ijms242417596. Int J Mol Sci. 2023. PMID: 38139422 Free PMC article.
-
The Role of Interleukin-10 in the Pathogenesis and Treatment of a Spinal Cord Injury.Diagnostics (Basel). 2024 Jan 9;14(2):151. doi: 10.3390/diagnostics14020151. Diagnostics (Basel). 2024. PMID: 38248028 Free PMC article. Review.
References
-
- Ali Z.S., Whitmore R.G. Surgical Intensive Care Medicine. 3rd ed. Springer; Berlin/Heidelberg, Germany: 2021. Spinal Cord Injuries; pp. 181–193. - DOI
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
