

Immune-Mediated Neuropathies: Pathophysiology and Management
- PMID: 37108447
- PMCID: PMC10139406
- DOI: 10.3390/ijms24087288
Immune-Mediated Neuropathies: Pathophysiology and Management
Abstract
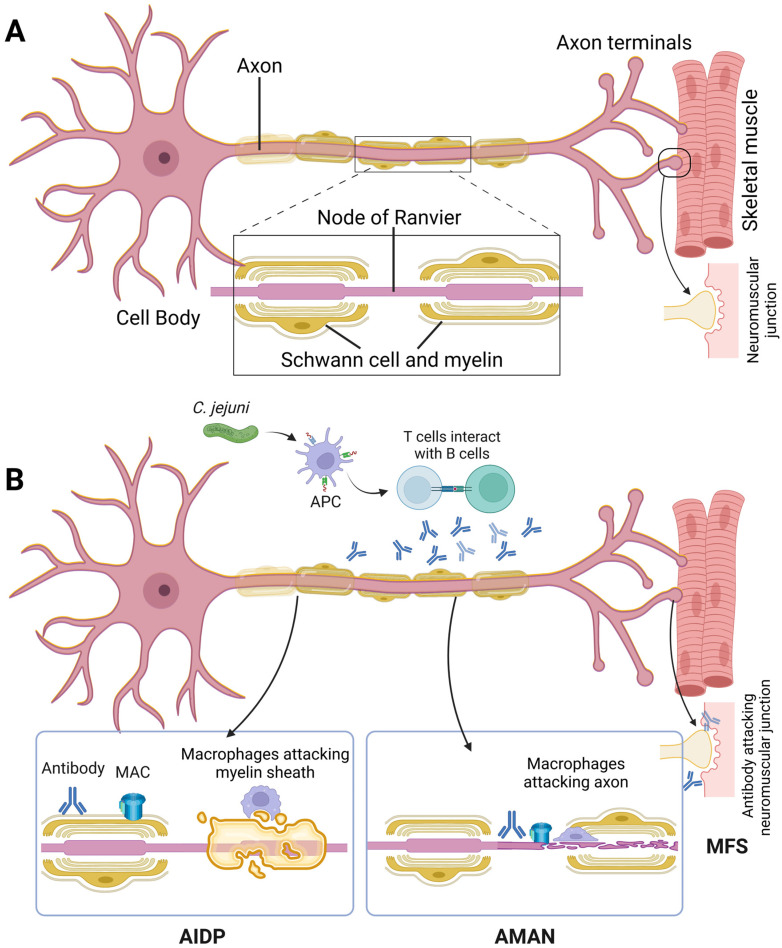
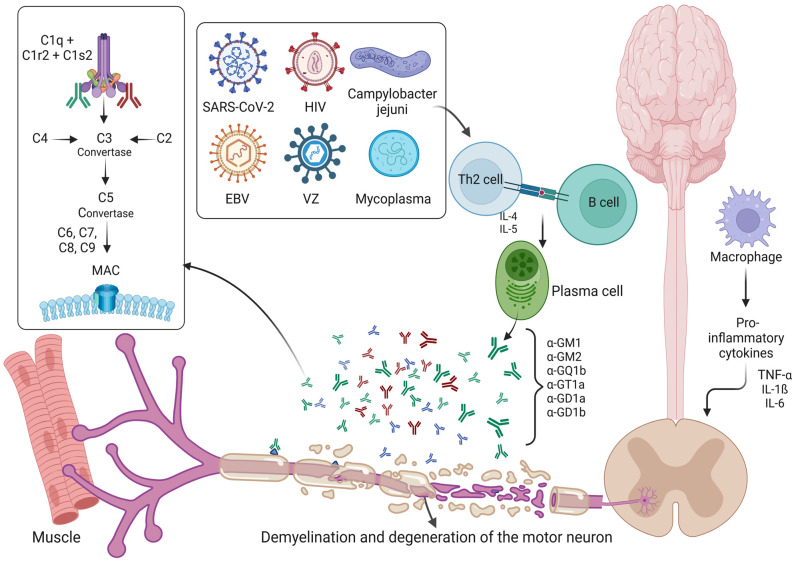
Dysfunction of the immune system can result in damage of the peripheral nervous system. The immunological mechanisms, which include macrophage infiltration, inflammation and proliferation of Schwann cells, result in variable degrees of demyelination and axonal degeneration. Aetiology is diverse and, in some cases, may be precipitated by infection. Various animal models have contributed and helped to elucidate the pathophysiological mechanisms in acute and chronic inflammatory polyradiculoneuropathies (Guillain-Barre Syndrome and chronic inflammatory demyelinating polyradiculoneuropathy, respectively). The presence of specific anti-glycoconjugate antibodies indicates an underlying process of molecular mimicry and sometimes assists in the classification of these disorders, which often merely supports the clinical diagnosis. Now, the electrophysiological presence of conduction blocks is another important factor in characterizing another subgroup of treatable motor neuropathies (multifocal motor neuropathy with conduction block), which is distinct from Lewis-Sumner syndrome (multifocal acquired demyelinating sensory and motor neuropathy) in its response to treatment modalities as well as electrophysiological features. Furthermore, paraneoplastic neuropathies are also immune-mediated and are the result of an immune reaction to tumour cells that express onconeural antigens and mimic molecules expressed on the surface of neurons. The detection of specific paraneoplastic antibodies often assists the clinician in the investigation of an underlying, sometimes specific, malignancy. This review aims to discuss the immunological and pathophysiological mechanisms that are thought to be crucial in the aetiology of dysimmune neuropathies as well as their individual electrophysiological characteristics, their laboratory features and existing treatment options. Here, we aim to present a balance of discussion from these diverse angles that may be helpful in categorizing disease and establishing prognosis.
Keywords: autoantibodies; demyelination; immunity; inflammation; neuropathy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Guillain G., Barre J.A., Strohl A. Radiculoneuritis Syndrome with Hyperalbuminosis of Cerebrospinal Fluid without Cellular Reaction. Notes on Clinical Features and Graphs of Tendon Reflexes. 1916. Ann. Med. Interne (Paris) 1999;150:24–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
