

Harnessing the Immunological Effects of Radiation to Improve Immunotherapies in Cancer
- PMID: 37108522
- PMCID: PMC10138513
- DOI: 10.3390/ijms24087359
Harnessing the Immunological Effects of Radiation to Improve Immunotherapies in Cancer
Abstract
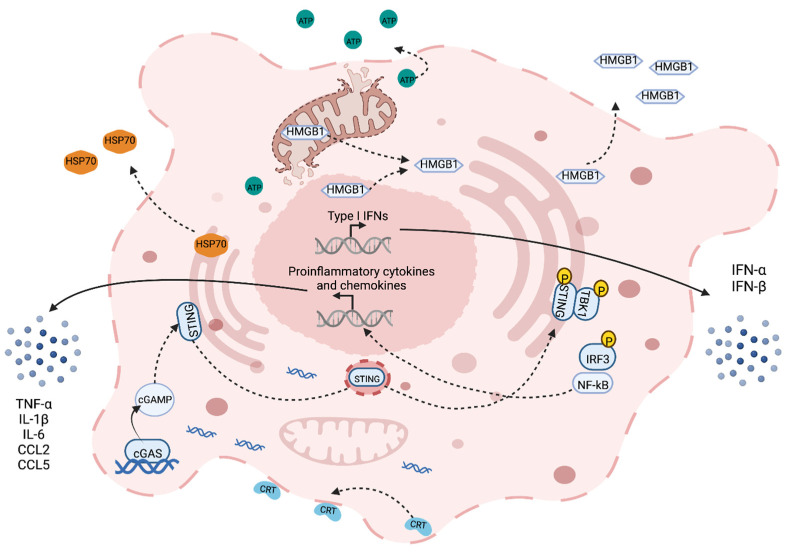
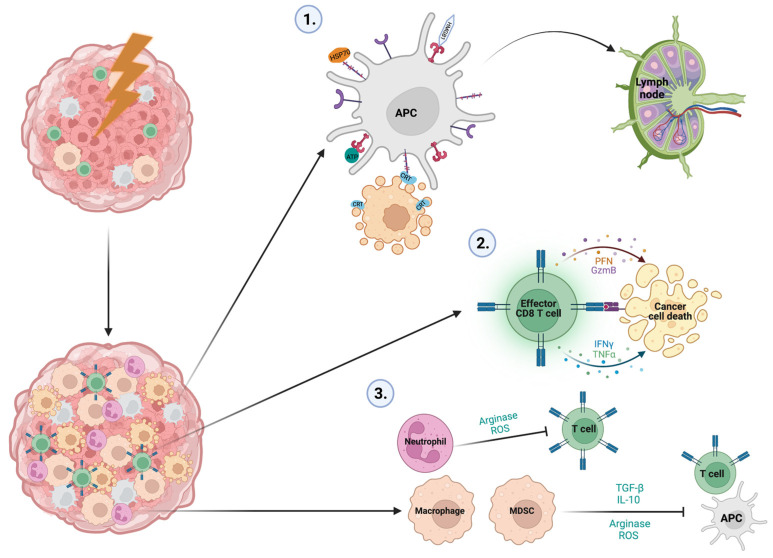
Ionizing radiation (IR) is used to treat 50% of cancers. While the cytotoxic effects related to DNA damage with IR have been known since the early 20th century, the role of the immune system in the treatment response is still yet to be fully determined. IR can induce immunogenic cell death (ICD), which activates innate and adaptive immunity against the cancer. It has also been widely reported that an intact immune system is essential to IR efficacy. However, this response is typically transient, and wound healing processes also become upregulated, dampening early immunological efforts to overcome the disease. This immune suppression involves many complex cellular and molecular mechanisms that ultimately result in the generation of radioresistance in many cases. Understanding the mechanisms behind these responses is challenging as the effects are extensive and often occur simultaneously within the tumor. Here, we describe the effects of IR on the immune landscape of tumors. ICD, along with myeloid and lymphoid responses to IR, are discussed, with the hope of shedding light on the complex immune stimulatory and immunosuppressive responses involved with this cornerstone cancer treatment. Leveraging these immunological effects can provide a platform for improving immunotherapy efficacy in the future.
Keywords: cancer; immunity; immunogenic cell death; immunotherapies; radiation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Department of Health Radiotherapy Services in England. [(accessed on 12 April 2023)];2012 Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploa....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
