

Coronary Artery Spasm-Related Heart Failure Syndrome: Literature Review
- PMID: 37108691
- PMCID: PMC10145866
- DOI: 10.3390/ijms24087530
Coronary Artery Spasm-Related Heart Failure Syndrome: Literature Review
Abstract
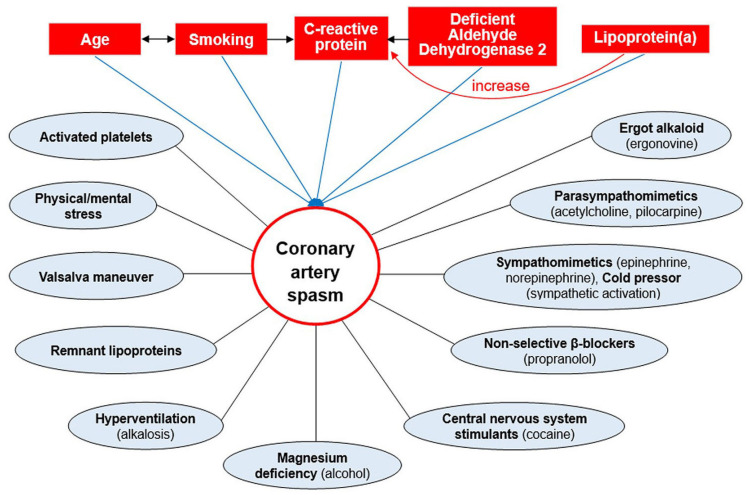
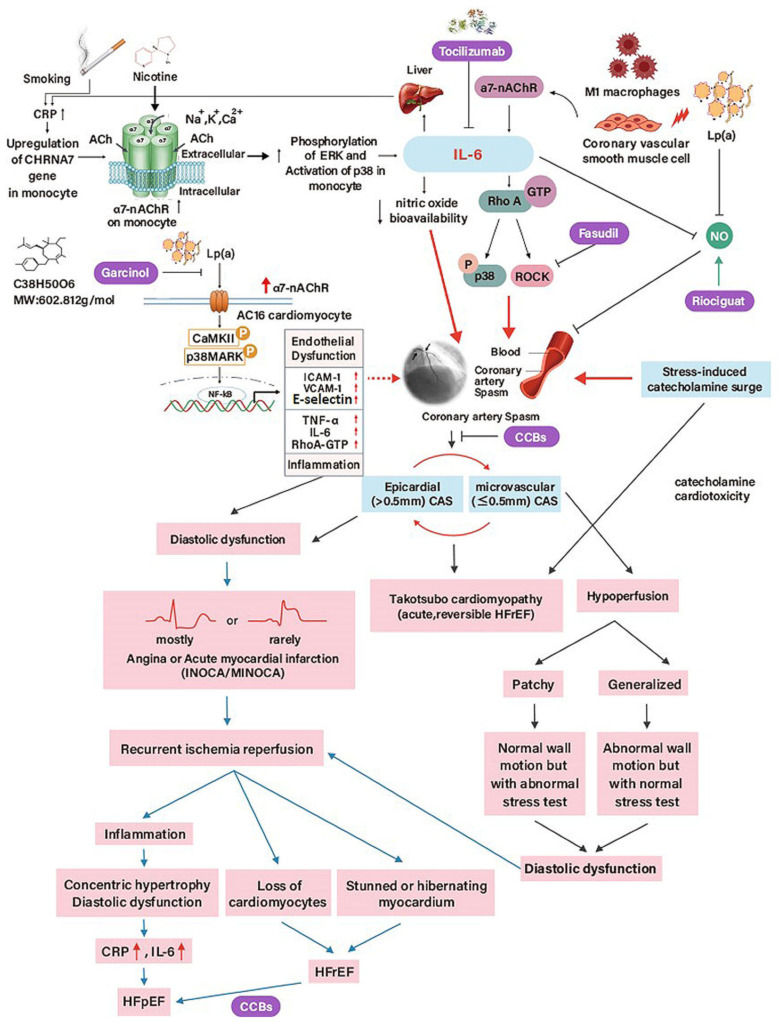
Although heart failure (HF) is a clinical syndrome that becomes worse over time, certain cases can be reversed with appropriate treatments. While coronary artery spasm (CAS) is still underappreciated and may be misdiagnosed, ischemia due to coronary artery disease and CAS is becoming the single most frequent cause of HF worldwide. CAS could lead to syncope, HF, arrhythmias, and myocardial ischemic syndromes such as asymptomatic ischemia, rest and/or effort angina, myocardial infarction, and sudden death. Albeit the clinical significance of asymptomatic CAS has been undervalued, affected individuals compared with those with classic Heberden's angina pectoris are at higher risk of syncope, life-threatening arrhythmias, and sudden death. As a result, a prompt diagnosis implements appropriate treatment strategies, which have significant life-changing consequences to prevent CAS-related complications, such as HF. Although an accurate diagnosis depends mainly on coronary angiography and provocative testing, clinical characteristics may help decision-making. Because the majority of CAS-related HF (CASHF) patients present with less severe phenotypes than overt HF, it underscores the importance of understanding risk factors correlated with CAS to prevent the future burden of HF. This narrative literature review summarises and discusses separately the epidemiology, clinical features, pathophysiology, and management of patients with CASHF.
Keywords: coronary artery spasm; heart failure with preserved ejection fraction; heart failure with reduced ejection fraction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
