

Preserving Ambulation in a Gene Therapy-Treated Girl Affected by Metachromatic Leukodystrophy: A Case Report
- PMID: 37109023
- PMCID: PMC10144348
- DOI: 10.3390/jpm13040637
Preserving Ambulation in a Gene Therapy-Treated Girl Affected by Metachromatic Leukodystrophy: A Case Report
Abstract
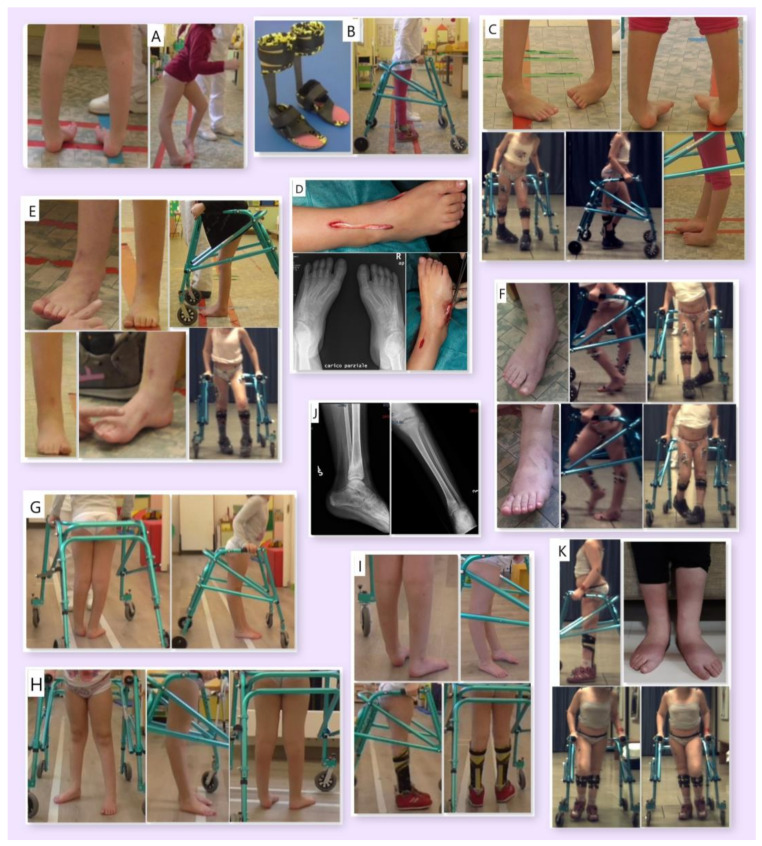
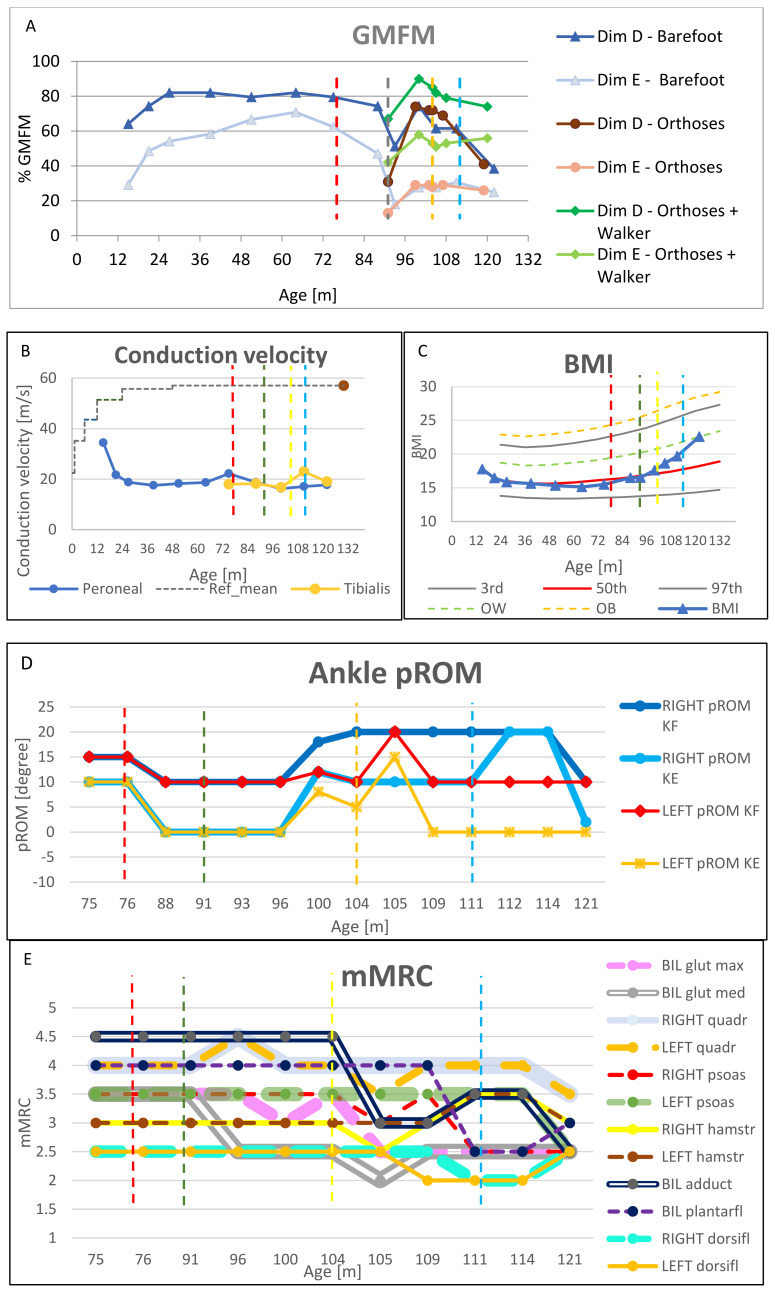
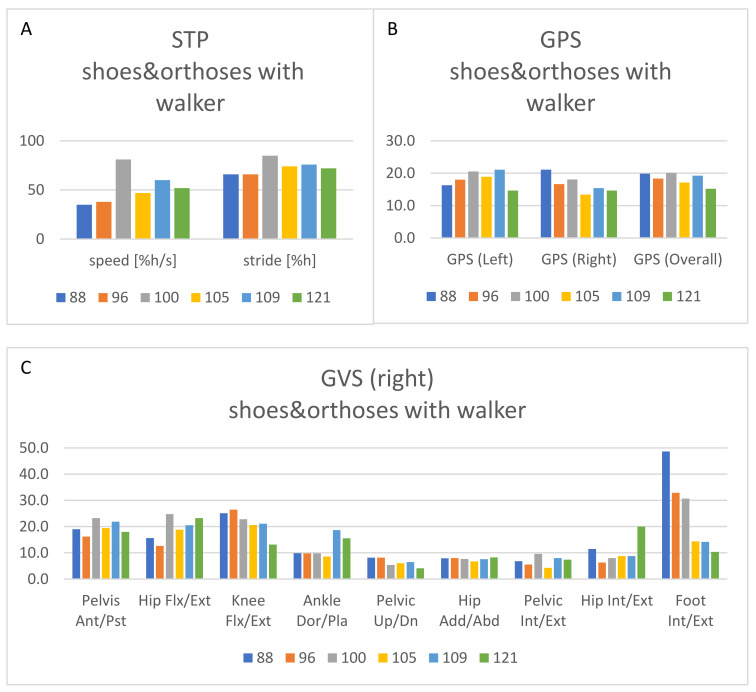
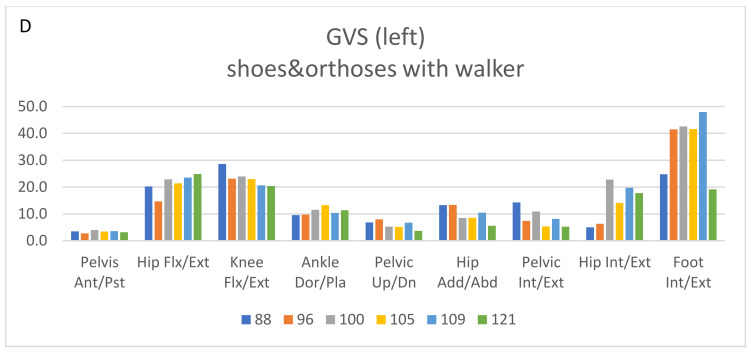
(1) Background: Atidarsagene autotemcel is a hematopoietic stem and progenitor cell gene therapy (HSPC-GT) approved to treat early-onset metachromatic leukodystrophy (MLD). The purpose of this case report is to describe the long-term management of residual gait impairment of a child with late infantile MLD treated with HSPC-GT. (2) Methods: Assessment included Gross Motor Function Measure-88, nerve conduction study, body mass index (BMI), Modified Tardieu Scale, passive range of motion, modified Medical Research Council scale, and gait analysis. Interventions included orthoses, a walker, orthopedic surgery, physiotherapy, and botulinum. (3) Results: Orthoses and a walker were fundamental to maintaining ambulation. Orthopedic surgery positively influenced gait by reducing equinovarus. Nonetheless, unilateral recurrence of varo-supination was observed, attributable to spasticity and muscle imbalance. Botulinum improved foot alignment but induced transient overall weakness. A significant increase in BMI occurred. Finally, a shift to bilateral valgopronation was observed, more easily managed with orthoses. (4) Conclusions: HSPC-GT preserved survival and locomotor abilities. Rehabilitation was then considered fundamental as a complementary treatment. Muscle imbalance and increased BMI contributed to gait deterioration in the growing phase. Caution is recommended when considering botulinum in similar subjects, as the risk of inducing overall weakness can outweigh the benefits of spasticity reduction.
Keywords: assistive devices; botulinum toxins; disabled children; gait analysis; muscle spasticity; nerve conduction studies; orthopedics; rehabilitation.
Conflict of interest statement
S.F., S.S. (Silvia Sassi), D.P., C.B. (Corrado Borghi), V.M., M.S., S.S. (Stefano Scarparo), and C.B. (Carla Butera) certify that they have no conflict of interest with any financial organization regarding the material discussed in the manuscript. The patient presented in the manuscript had previously been enrolled in the clinical trial
Figures
References
-
- Kehrer C., Elgün S., Raabe C., Böhringer J., Beck-Wödl S., Bevot A., Kaiser N., Schöls L., Krägeloh-Mann I., Groeschel S. Association of Age at Onset and First Symptoms With Disease Progression in Patients With Metachromatic Leukodystrophy. Neurology. 2020;96:e255–e266. doi: 10.1212/WNL.0000000000011047. - DOI - PubMed
-
- Artigalás O., Lagranha V.L., Saraiva-Pereira M.L., Burin M.G., Lourenço C.M., van der Linden H., Jr., Santos M.L.F., Rosemberg S., Steiner C.E., Kok F., et al. Clinical and biochemical study of 29 Brazilian patients with metachromatic leukodystrophy. J. Inherit. Metab. Dis. 2010;33((Suppl. 3)):S257–S262. doi: 10.1007/s10545-010-9140-4. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
