

Continuing Challenges in the Definitive Diagnosis of Cushing's Disease: A Structured Review Focusing on Molecular Imaging and a Proposal for Diagnostic Work-Up
- PMID: 37109254
- PMCID: PMC10144206
- DOI: 10.3390/jcm12082919
Continuing Challenges in the Definitive Diagnosis of Cushing's Disease: A Structured Review Focusing on Molecular Imaging and a Proposal for Diagnostic Work-Up
Abstract
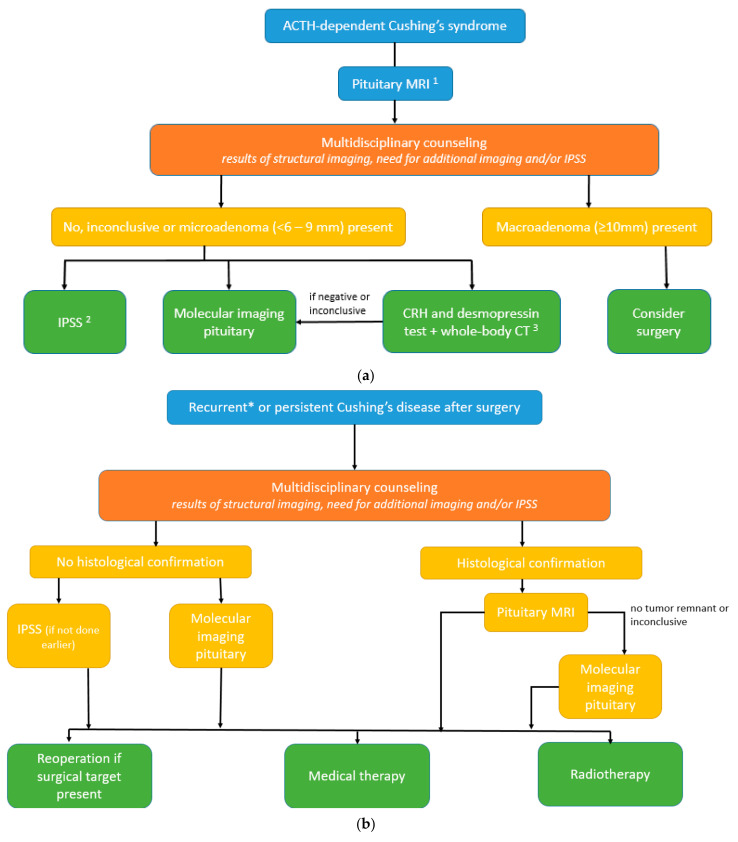
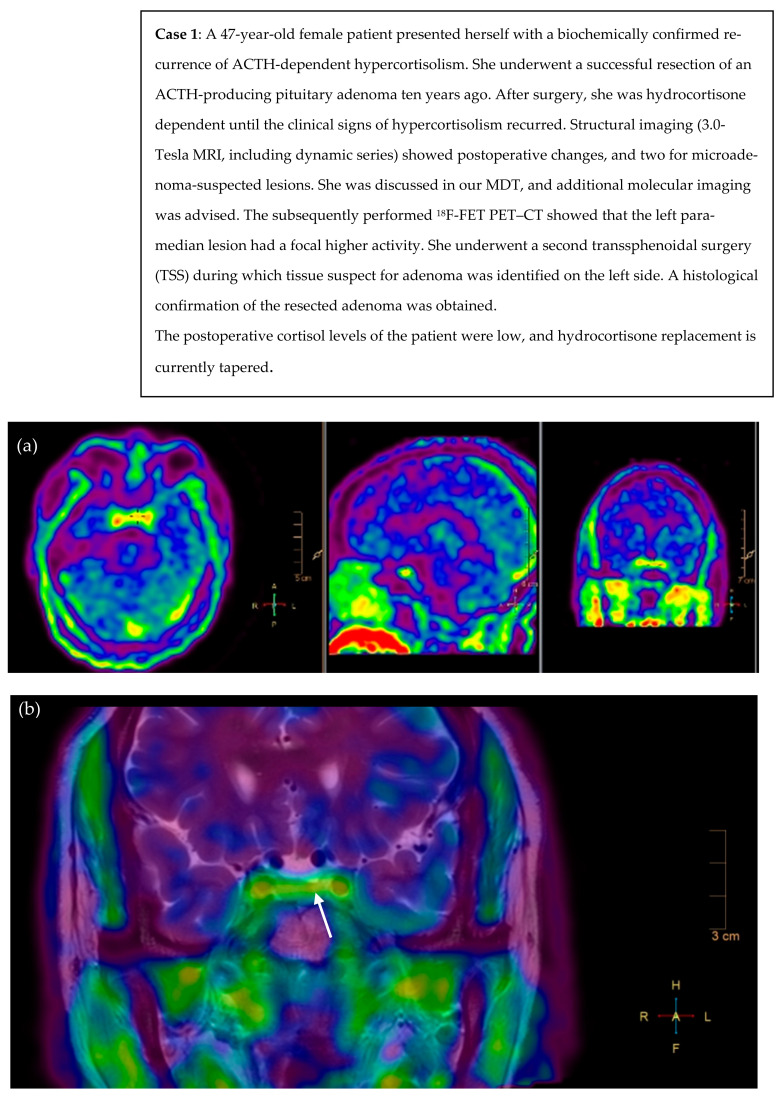
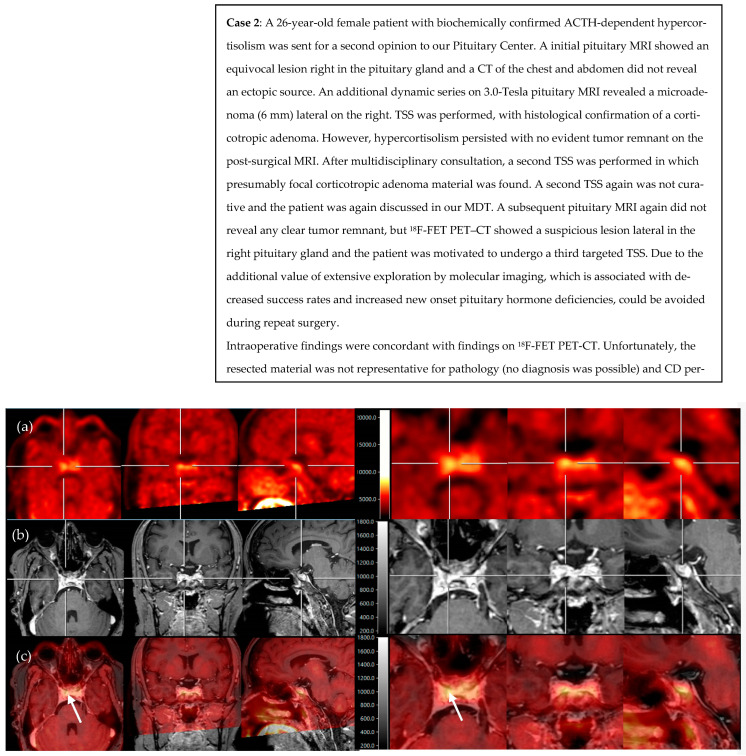
The definitive diagnosis of Cushing's disease (CD) in the presence of pituitary microadenoma remains a continuous challenge. Novel available pituitary imaging techniques are emerging. This study aimed to provide a structured analysis of the diagnostic accuracy as well as the clinical use of molecular imaging in patients with ACTH-dependent Cushing's syndrome (CS). We also discuss the role of multidisciplinary counseling in decision making. Additionally, we propose a complementary diagnostic algorithm for both de novo and recurrent or persistent CD. A structured literature search was conducted and two illustrative CD cases discussed at our Pituitary Center are presented. A total of 14 CD (n = 201) and 30 ectopic CS (n = 301) articles were included. MRI was negative or inconclusive in a quarter of CD patients. 11C-Met showed higher pituitary adenoma detection than 18F-FDG PET-CT (87% versus 49%). Up to 100% detection rates were found for 18F-FET, 68Ga-DOTA-TATE, and 68Ga-DOTA-CRH, but were based on single studies. The use of molecular imaging modalities in the detection of pituitary microadenoma in ACTH-dependent CS is of added and complementary value, serving as one of the available tools in the diagnostic work-up. In selected CD cases, it seems justified to even refrain from IPSS.
Keywords: Cushing’s disease; PET; diagnosis; hypercortisolism; molecular imaging; pituitary.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Arnaldi G., Angeli A., Atkinson A.B., Bertagna X., Cavagnini F., Chrousos G.P., Fava G.A., Findling J.W., Gaillard R.C., Grossman A.B., et al. Diagnosis and Complications of Cushing’s Syndrome: A Consensus Statement. J. Clin. Endocrinol. Metab. 2003;88:5593–5602. doi: 10.1210/jc.2003-030871. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
