

Update on Shoulder Arthroplasties with Emphasis on Imaging
- PMID: 37109282
- PMCID: PMC10143235
- DOI: 10.3390/jcm12082946
Update on Shoulder Arthroplasties with Emphasis on Imaging
Abstract
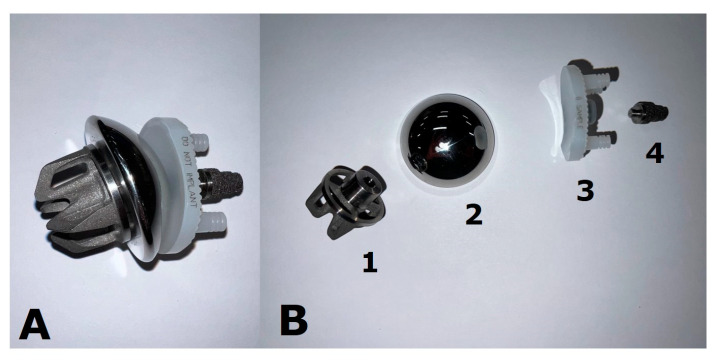
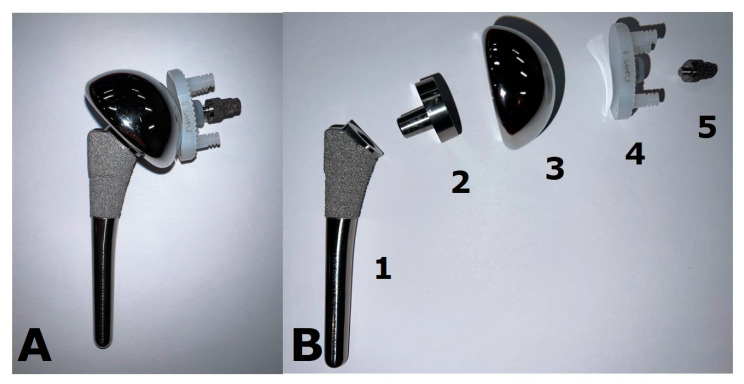
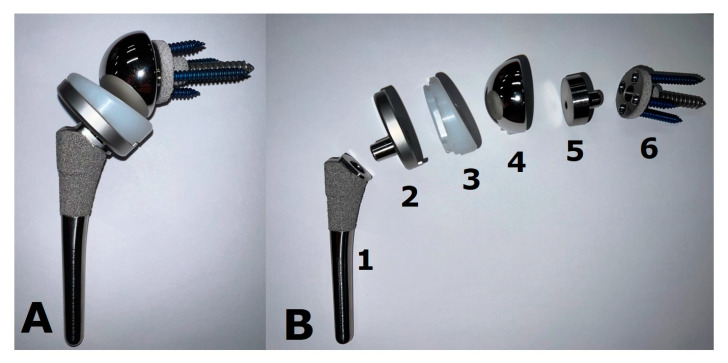
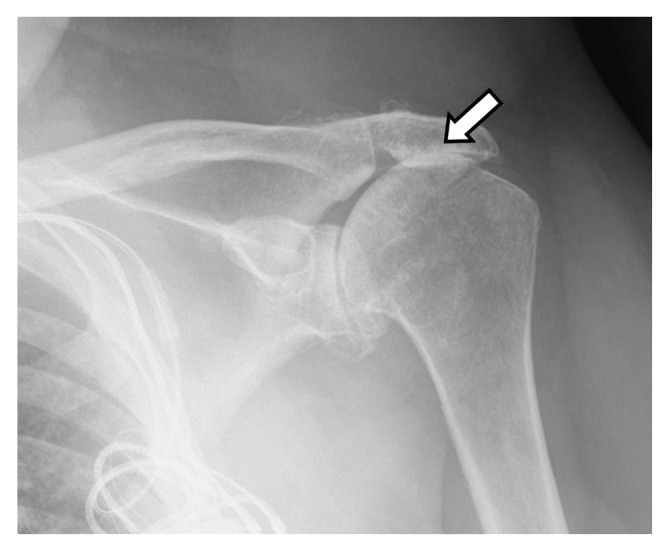
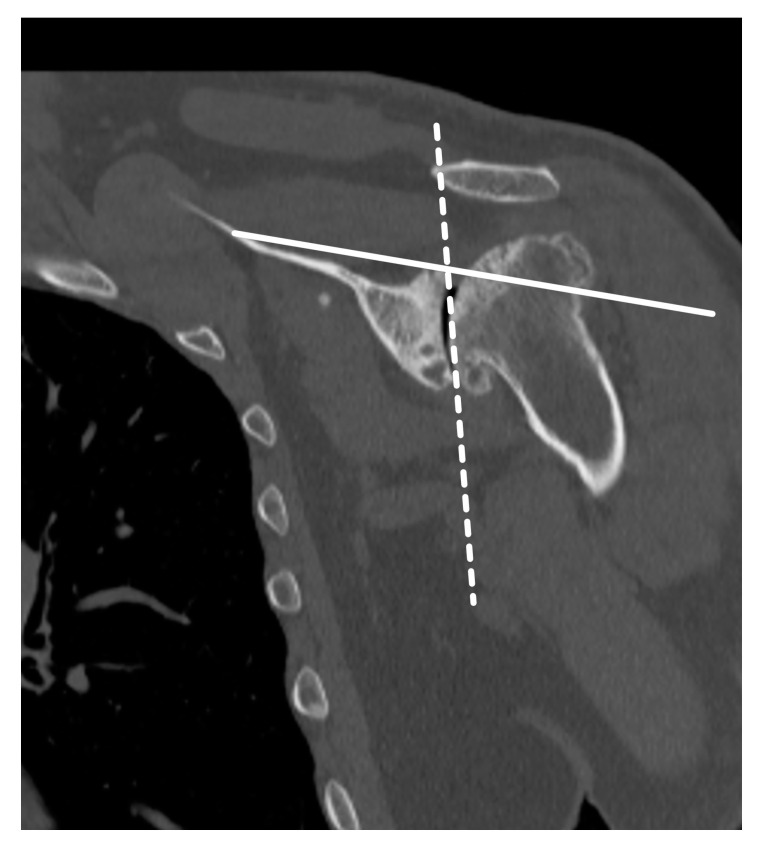
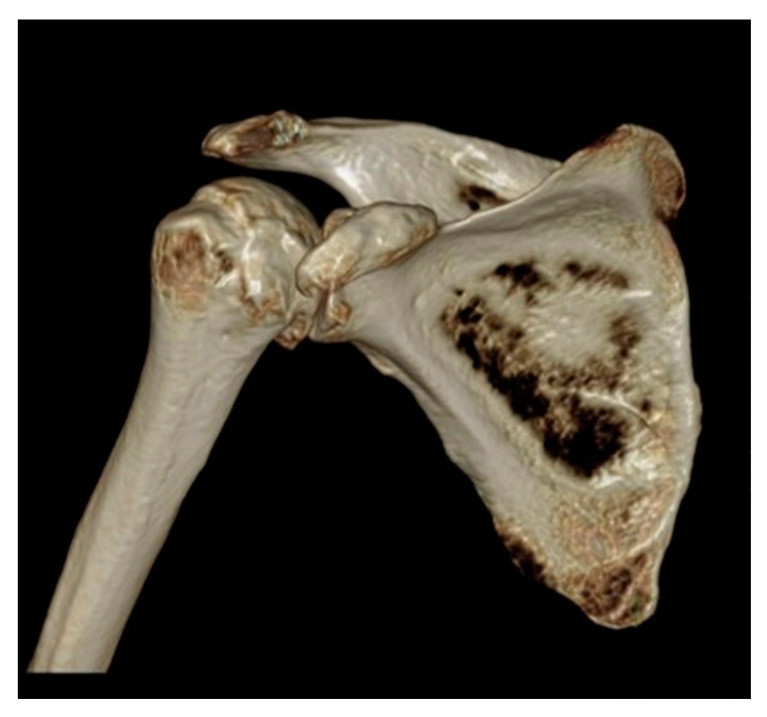
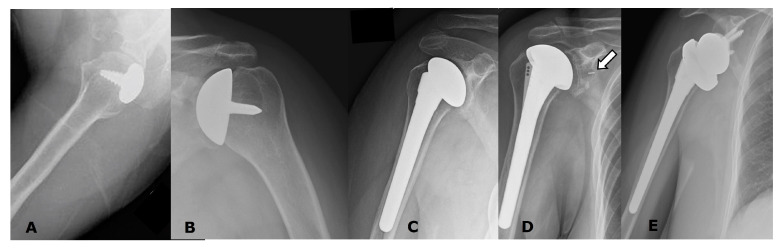
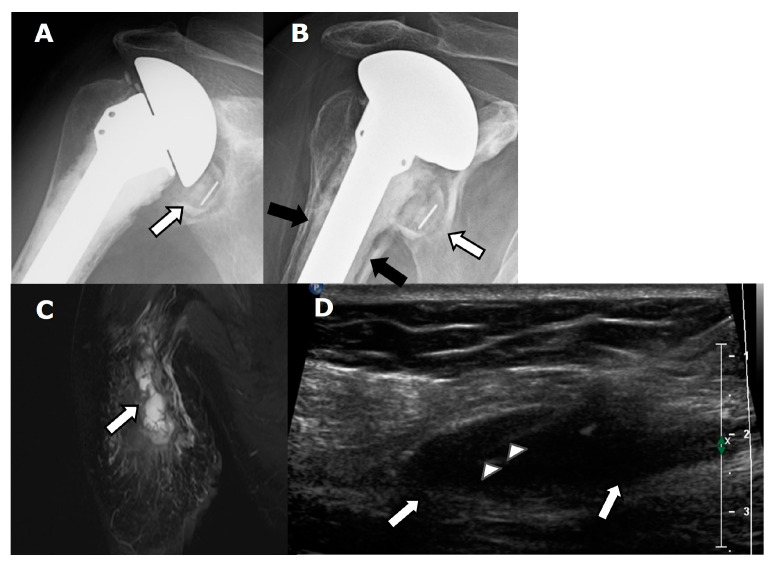
Shoulder pain and dysfunction may significantly impact quality of life. If conservative measures fail, advanced disease is frequently treated with shoulder arthroplasty, which is currently the third most common joint replacement surgery following the hip and knee. The main indications for shoulder arthroplasty include primary osteoarthritis, post-traumatic arthritis, inflammatory arthritis, osteonecrosis, proximal humeral fracture sequelae, severely dislocated proximal humeral fractures, and advanced rotator cuff disease. Several types of anatomic arthroplasties are available, such as humeral head resurfacing and hemiarthroplasties, as well as total anatomic arthroplasties. Reverse total shoulder arthroplasties, which reverse the normal ball-and-socket geometry of the shoulder, are also available. Each of these arthroplasty types has specific indications and unique complications in addition to general hardware-related or surgery-related complications. Imaging-including radiography, ultrasonography, computed tomography, magnetic resonance imaging, and, occasionally, nuclear medicine imaging-has a key role in the initial pre-operative evaluation for shoulder arthroplasty, as well as in post-surgical follow-up. This review paper aims to discuss important pre-operative imaging considerations, including rotator cuff evaluation, glenoid morphology, and glenoid version, as well as to review post-operative imaging of the various types of shoulder arthroplasties, to include normal post-operative appearances as well as imaging findings of complications.
Keywords: arthritis; arthroplasty; computed tomography; magnetic resonance imaging; radiography; rotator cuff; shoulder; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
