

Effect of Exercise on Liver Function and Insulin Resistance Markers in Patients with Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 37109347
- PMCID: PMC10143548
- DOI: 10.3390/jcm12083011
Effect of Exercise on Liver Function and Insulin Resistance Markers in Patients with Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Background: Structured exercise as part of lifestyle modification plays an important role in the improvement of non-alcoholic fatty liver disease (NAFLD); however, its effectiveness has been shown to vary. This systematic review with meta-analysis investigated the effects of exercise on liver function and insulin resistance markers in patients with NAFLD.
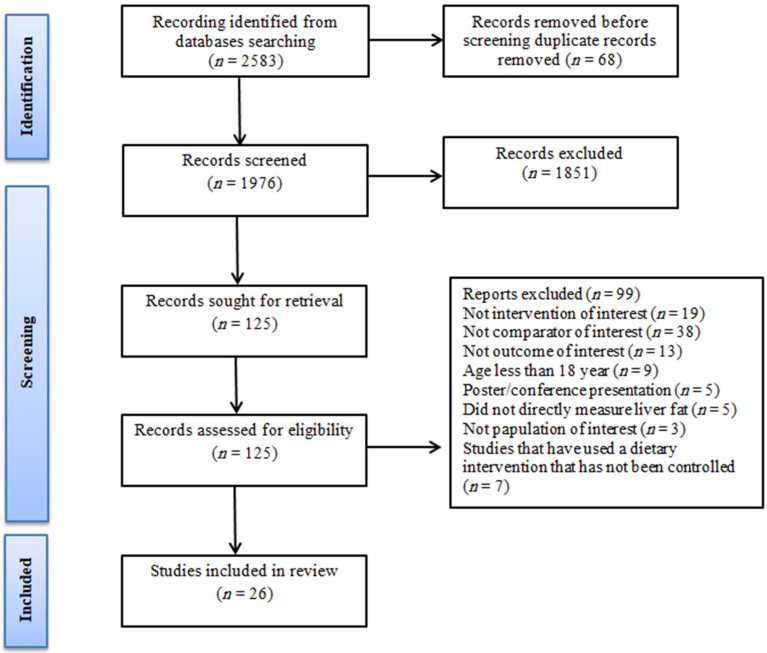
Methods: Six electronic databases were searched using terms related to exercise and NAFLD up to March 2022. Data were analyzed using a random-effects model to estimate the standardized mean difference (SMD) and 95% confidence interval.
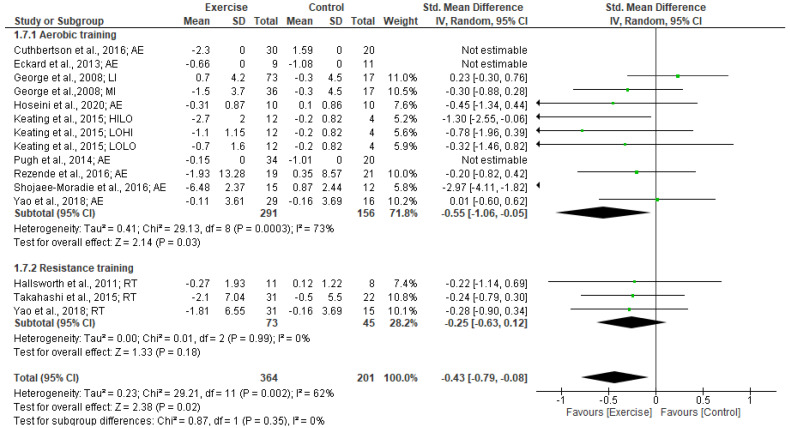
Results: The systematic search identified 2583 articles, of which a total of 26 studies met the inclusion criteria and were eligible. Exercise training had a moderate effect on reducing ALT (SMD: -0.59, p = 0.01) and small effects on reducing AST (SMD: -0.40, p = 0.01) and insulin (SMD: -0.43, p = 0.02). Significant reductions in ALT were found following aerobic training (SMD: -0.63, p < 0.01) and resistance training (SMD: -0.45, p < 0.001). Moreover, reductions in AST were found following resistance training (SMD: -0.54, p = 0.001), but not after aerobic training and combined training. However, reductions in insulin were found following aerobic training (SMD: -0.55, p = 0.03). Exercise interventions for <12 weeks compared to ≥12 weeks were more effective in reducing FBG and HOMA-IR, while interventions for ≥12 weeks compared to <12 weeks were more effective in reducing ALT and AST levels.
Conclusions: Our findings support the effectiveness of exercise in improving liver function markers but not in blood glucose control in NAFLD patients. Additional studies are needed to determine the exercise prescription to maximize health in these patients.
Keywords: exercise training; insulin resistance; liver enzymes; meta-analysis; non-alcoholic fatty liver disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
