

Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases-Diagnosis and Treatment
- PMID: 37111344
- PMCID: PMC10141986
- DOI: 10.3390/ph16040587
Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases-Diagnosis and Treatment
Abstract
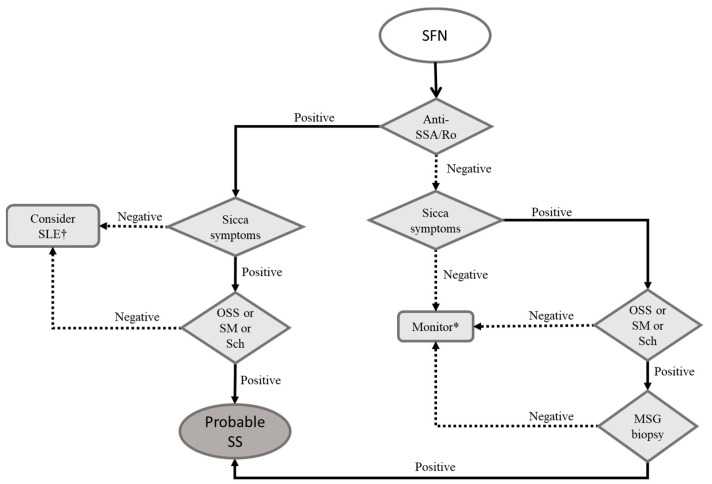
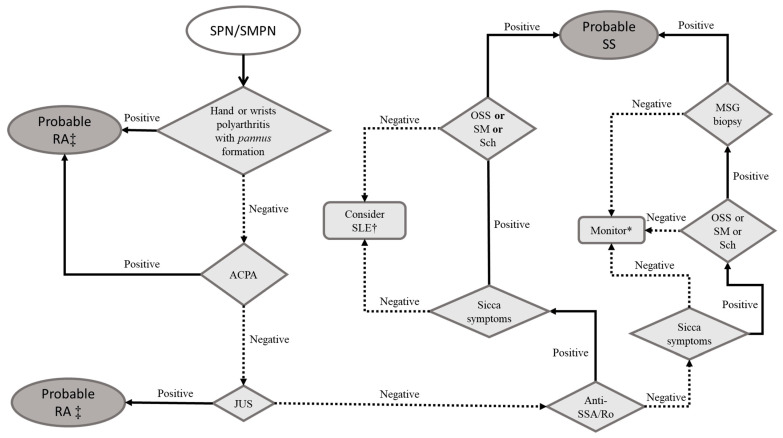
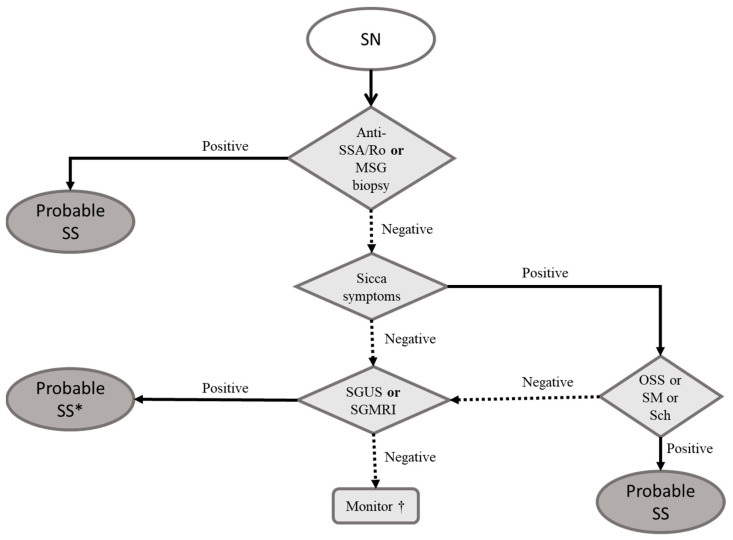
Peripheral neuropathy (PN) is frequently observed in systemic rheumatic diseases and is a challenge in clinical practice. We aimed to review the evidence on the subject and proposed a comprehensive approach to these patients, facilitating diagnosis and management. We searched the MEDLINE database for the terms (and its respective Medical Subject Headings (MeSH) terms): "peripheral neuropathy" AND "rheumatic diseases" OR "systemic lupus erythematosus", "rheumatoid arthritis", "Sjogren syndrome", and "vasculitis" from 2000 to 2023. This literature review focuses on the diagnostic workup of PNs related to systemic lupus erythematosus, Sjögren's syndrome, rheumatoid arthritis, and systemic vasculitis. For every type of PN, we provide a pragmatic flowchart for diagnosis and also describe evidence-based strategies of treatment.
Keywords: connective tissue diseases; peripheral neuropathy; rheumatic diseases; systemic vasculitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Central Nervous System Involvement in Systemic Autoimmune Rheumatic Diseases-Diagnosis and Treatment.Pharmaceuticals (Basel). 2024 Aug 7;17(8):1044. doi: 10.3390/ph17081044. Pharmaceuticals (Basel). 2024. PMID: 39204149 Free PMC article. Review.
-
Motor neuron disease in a patient with overlap syndrome (rheumatoid arthritis; systemic lupus erythematosus, Sjogren's syndrome).Rheumatol Int. 2023 Feb;43(2):367-372. doi: 10.1007/s00296-022-05207-z. Epub 2022 Sep 18. Rheumatol Int. 2023. PMID: 36117188 Free PMC article. Review.
-
Connective tissue disorders: systemic lupus erythematosus, Sjögren's syndrome, and scleroderma.Handb Clin Neurol. 2014;119:463-73. doi: 10.1016/B978-0-7020-4086-3.00030-8. Handb Clin Neurol. 2014. PMID: 24365313 Review.
-
Suspected inflammatory rheumatic diseases in patients presenting with skin rashes.Best Pract Res Clin Rheumatol. 2019 Aug;33(4):101440. doi: 10.1016/j.berh.2019.101440. Epub 2019 Oct 1. Best Pract Res Clin Rheumatol. 2019. PMID: 31585842 Review.
-
[Difficulties in differential diagnosis of Sjögren's syndrome and systemic lupus erythematosus].Przegl Lek. 2006;63(5):278-83. Przegl Lek. 2006. PMID: 17036505 Review. Polish.
Cited by
-
Cerebrovascular Involvement in Systemic Sclerosis.ACR Open Rheumatol. 2025 Apr;7(4):e70032. doi: 10.1002/acr2.70032. ACR Open Rheumatol. 2025. PMID: 40223737 Free PMC article. Review.
-
Prevalence of Subclinical Peripheral Neuropathy in Patients With Autoimmune Connective Tissue Disorders: An Observational Cross-Sectional Study.Cureus. 2024 Sep 26;16(9):e70294. doi: 10.7759/cureus.70294. eCollection 2024 Sep. Cureus. 2024. PMID: 39469412 Free PMC article.
-
Central Nervous System Involvement in Systemic Autoimmune Rheumatic Diseases-Diagnosis and Treatment.Pharmaceuticals (Basel). 2024 Aug 7;17(8):1044. doi: 10.3390/ph17081044. Pharmaceuticals (Basel). 2024. PMID: 39204149 Free PMC article. Review.
-
Unveiling the Role of Nerve Conduction Studies (NCS) in Detecting Subclinical Peripheral Neuropathy in Autoimmune Disorders: A Cross-Sectional Study.Cureus. 2024 Oct 1;16(10):e70649. doi: 10.7759/cureus.70649. eCollection 2024 Oct. Cureus. 2024. PMID: 39483557 Free PMC article.
-
Polyneuropathy in systemic sclerosis: exploring the causes and biomarkers.Front Med (Lausanne). 2024 Aug 2;11:1412706. doi: 10.3389/fmed.2024.1412706. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39156689 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
