

Cancer Resistance to Immunotherapy: Comprehensive Insights with Future Perspectives
- PMID: 37111629
- PMCID: PMC10141036
- DOI: 10.3390/pharmaceutics15041143
Cancer Resistance to Immunotherapy: Comprehensive Insights with Future Perspectives
Abstract
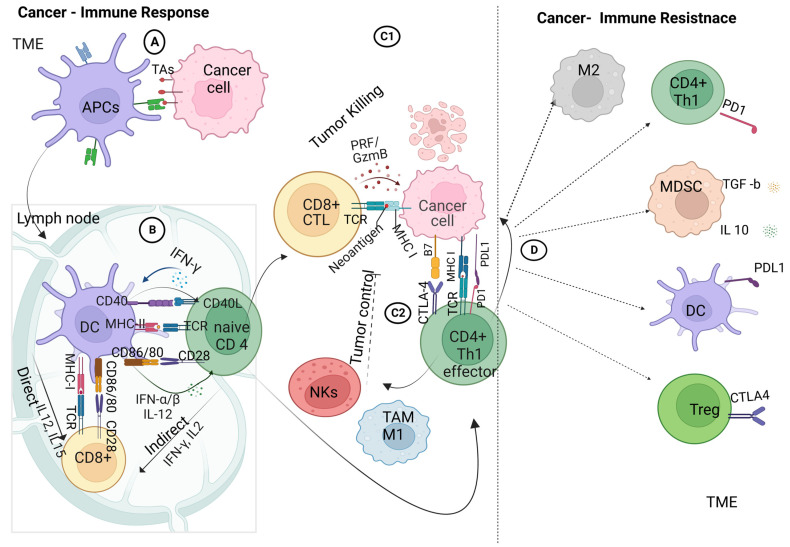
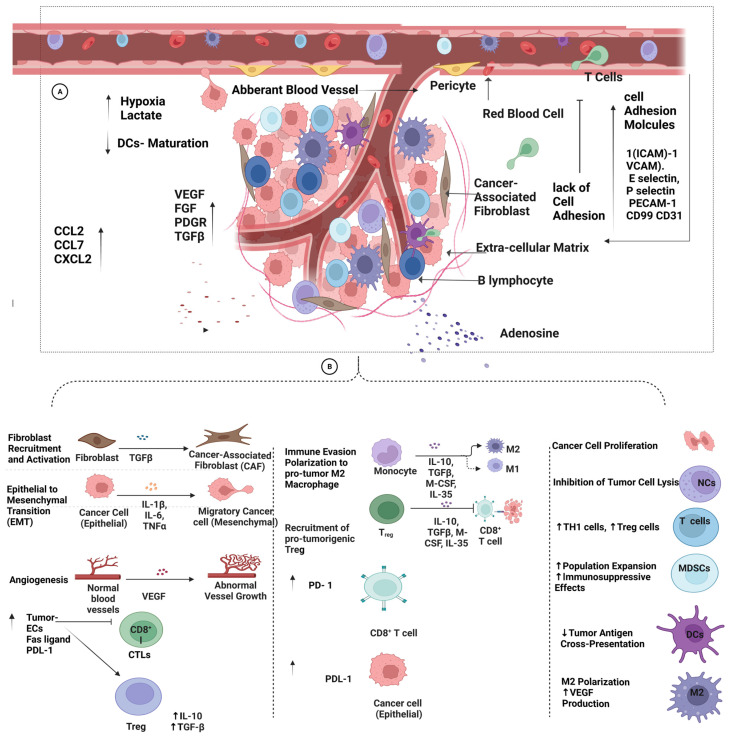
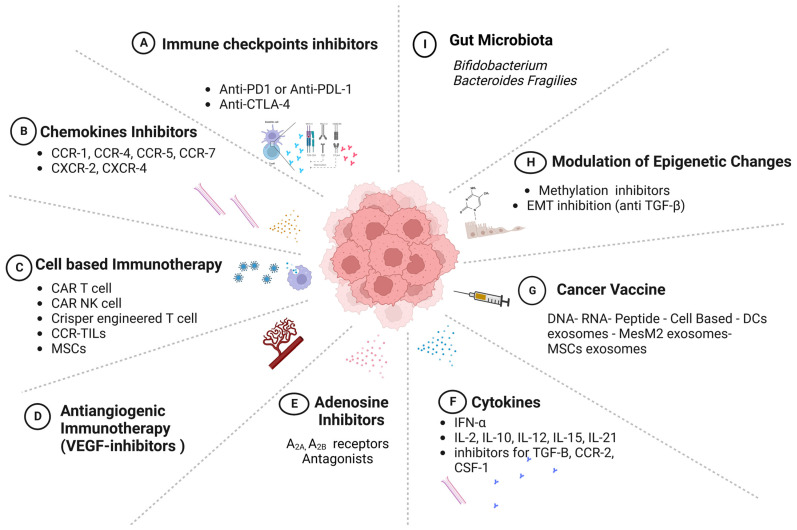
Cancer immunotherapy is a type of treatment that harnesses the power of the immune systems of patients to target cancer cells with better precision compared to traditional chemotherapy. Several lines of treatment have been approved by the US Food and Drug Administration (FDA) and have led to remarkable success in the treatment of solid tumors, such as melanoma and small-cell lung cancer. These immunotherapies include checkpoint inhibitors, cytokines, and vaccines, while the chimeric antigen receptor (CAR) T-cell treatment has shown better responses in hematological malignancies. Despite these breakthrough achievements, the response to treatment has been variable among patients, and only a small percentage of cancer patients gained from this treatment, depending on the histological type of tumor and other host factors. Cancer cells develop mechanisms to avoid interacting with immune cells in these circumstances, which has an adverse effect on how effectively they react to therapy. These mechanisms arise either due to intrinsic factors within cancer cells or due other cells within the tumor microenvironment (TME). When this scenario is used in a therapeutic setting, the term "resistance to immunotherapy" is applied; "primary resistance" denotes a failure to respond to treatment from the start, and "secondary resistance" denotes a relapse following the initial response to immunotherapy. Here, we provide a thorough summary of the internal and external mechanisms underlying tumor resistance to immunotherapy. Furthermore, a variety of immunotherapies are briefly discussed, along with recent developments that have been employed to prevent relapses following treatment, with a focus on upcoming initiatives to improve the efficacy of immunotherapy for cancer patients.
Keywords: cancer immunotherapy; immune checkpoint inhibitors; resistance; tumor microenvironment.
Conflict of interest statement
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.
Figures



References
-
- Wagner E., Elliot K., Enders W., Chobanuk J., Tsui A. BOOK REVIEW: Chemotherapy and Biotherapy Guidelines, and Recommendations for Practice 4th Edition. Can. Oncol. Nurs. J. Rev. Can. De Soins Infirm. En Oncol. 2015;25:480.
-
- Almajali B., Al-Jamal H.A.N., Wan Taib W.R., Ismail I., Johan M.F., Doolaanea A.A., Ibrahim W.N., Tajudin S.A. Thymoquinone Suppresses Cell Proliferation and Enhances Apoptosis of HL60 Leukemia Cells through Re-Expression of JAK/STAT Negative Regulators. Asian Pac. J. Cancer Prev. 2021;22:879–885. doi: 10.31557/apjcp.2021.22.3.879. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
