

Salivary Antibody Responses to Two COVID-19 Vaccines following Different Vaccination Regimens
- PMID: 37112657
- PMCID: PMC10146373
- DOI: 10.3390/vaccines11040744
Salivary Antibody Responses to Two COVID-19 Vaccines following Different Vaccination Regimens
Abstract
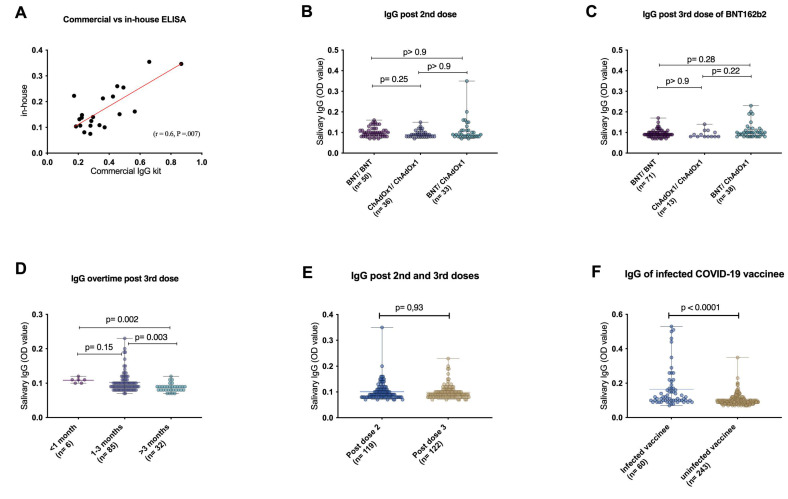
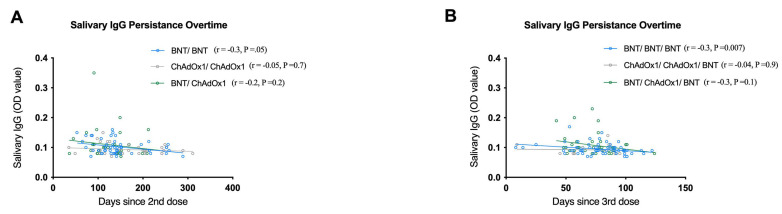
Background: To date, little is known about the salivary mucosal immune response following different COVID-19 vaccine types or after a booster (3rd) dose of the BNT162b2 (BNT) vaccine. Methods: A total of 301 saliva samples were collected from vaccinated individuals and arranged into two cohorts: cohort 1 (n = 145), samples from individuals who had received two doses against SARS-CoV-2; cohort 2 (n = 156), samples from individuals who had received a booster of BNT vaccine. Cohorts 1 and 2 were sub-stratified into three groups based on the types of first and second doses (homologous BNT/BNT, homologous ChAdOx1/ChAdOx1, or heterologous BNT/ChAdOx1vaccinations). Salivary immunoglobulin G (IgG) response to SARS-CoV-2 spike glycoprotein was measured by ELISA, and clinical demographic data were collected from hospital records or questionnaires. Results: Salivary IgG antibody responses against different vaccines, whether homologous or heterogeneous vaccination regimens, showed similar levels in cohorts 1 and 2. Compiling all groups in cohort 1 and 2 showed significant, albeit weak, negative correlations between salivary IgG levels and time (r = -0.2, p = 0.03; r = -0.27, p = 0.003, respectively). In cohort 2, the durability of salivary IgG after a booster dose of BNT162b2 significantly dropped after 3 months compared to the <1 month and 1-3 months groups. Conclusions: Different COVID-19 vaccine types and regimens elicit similar salivary anti-SARS-CoV-2 IgG with modest waning over time. Boosting with BNT162b2 vaccine did not produce an evident increase in mucosal IgG response whereby COVID-19 recovered subjects show higher salivary IgG than naive, post-vaccination subjects. The ChAdOx1/ChAdOx1 regimen showed better correlation between salivary IgG levels and durability. These findings highlight the importance of developing oral or intra-nasal vaccines to induce stronger mucosal immunity.
Keywords: COVID-19; ELISA; IgG; SARS-CoV-2; antibody; immune responses; mucosal; saliva; vaccines.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- University of Johns Hopkins Coronavirus Resource Center. [(accessed on 18 January 2023)]. Available online: https://coronavirus.jhu.edu/map.html.
-
- Haas E.J., Angulo F.J., McLaughlin J.M., Anis E., Singer S.R., Khan F., Brooks N., Smaja M., Mircus G., Pan K., et al. Impact and Effectiveness of MRNA BNT162b2 Vaccine against SARS-CoV-2 Infections and COVID-19 Cases, Hospitalisations, and Deaths Following a Nationwide Vaccination Campaign in Israel: An Observational Study Using National Surveillance Data. Lancet. 2021;397:1819–1829. doi: 10.1016/S0140-6736(21)00947-8. - DOI - PMC - PubMed
-
- Voysey M., Clemens S.A.C., Madhi S.A., Weckx L.Y., Folegatti P.M., Aley P.K., Angus B., Baillie V.L., Barnabas S.L., Bhorat Q.E., et al. Safety and Efficacy of the ChAdOx1 NCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet. 2021;397:99–111. doi: 10.1016/S0140-6736(20)32661-1. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
