

In-Depth Analysis of the Re-Emergence of Respiratory Syncytial Virus at a Tertiary Care Hospital in Germany in the Summer of 2021 after the Alleviation of Non-Pharmaceutical Interventions Due to the SARS-CoV-2 Pandemic
- PMID: 37112857
- PMCID: PMC10144477
- DOI: 10.3390/v15040877
In-Depth Analysis of the Re-Emergence of Respiratory Syncytial Virus at a Tertiary Care Hospital in Germany in the Summer of 2021 after the Alleviation of Non-Pharmaceutical Interventions Due to the SARS-CoV-2 Pandemic
Abstract
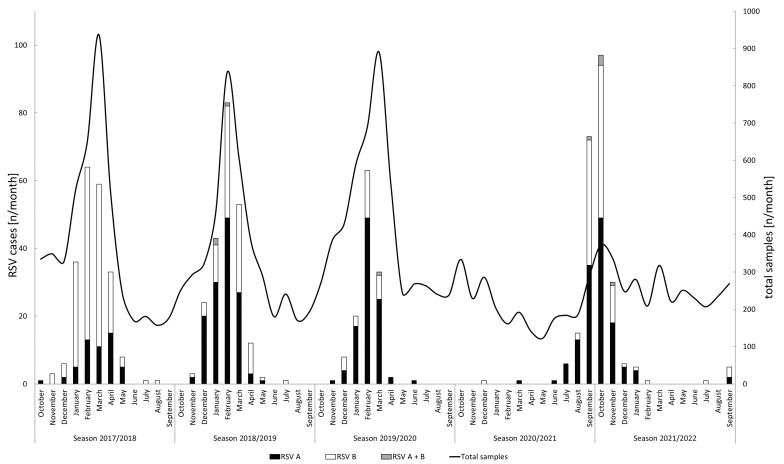
Following the extensive non-pharmaceutical interventions (NPIs) and behavioral changes in the wake of the SARS-CoV-2 pandemic, an interseasonal rise in respiratory syncytial virus (RSV) cases was observed in Germany in 2021. The aim of this study was to characterize the local molecular epidemiology of RSV infections in comparison to the three pre-pandemic seasons. Additionally, clinical data were retrieved from patient charts to determine the clinical significance of RSV infections. RSV detections peaked in calendar week 40 of 2021, 18 weeks earlier than the usual peak observed in the three pre-pandemic seasons. Sequence analysis revealed a close phylogenetic relatedness regardless of the season of origin. A significantly higher amount of pediatric cases (88.9% of all cases, p < 0.001) was observed for season 2021/2022. For the pediatric cases, significant differences were observed for an increased number of siblings in the household (p = 0.004), a lower rate of fever (p = 0.007), and a reduced amount of co-infections (p = 0.001). Although the mean age of the adult patients was significantly younger (47.1 vs. 64.7, p < 0.001), high rates of comorbidities, lower respiratory tract infections and intensive care unit admissions prevailed. The NPIs in the wake of the SARS-CoV-2 pandemic had a tremendous impact on the epidemiologic characteristics and seasonality of RSV and warrant further epidemiologic studies of this important pathogen.
Keywords: RSV; molecular epidemiology; non-pharmaceutical interventions; respiratory infections; respiratory viruses.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
