

SARS-CoV-2-Induced Myocarditis: A State-of-the-Art Review
- PMID: 37112896
- PMCID: PMC10145666
- DOI: 10.3390/v15040916
SARS-CoV-2-Induced Myocarditis: A State-of-the-Art Review
Abstract
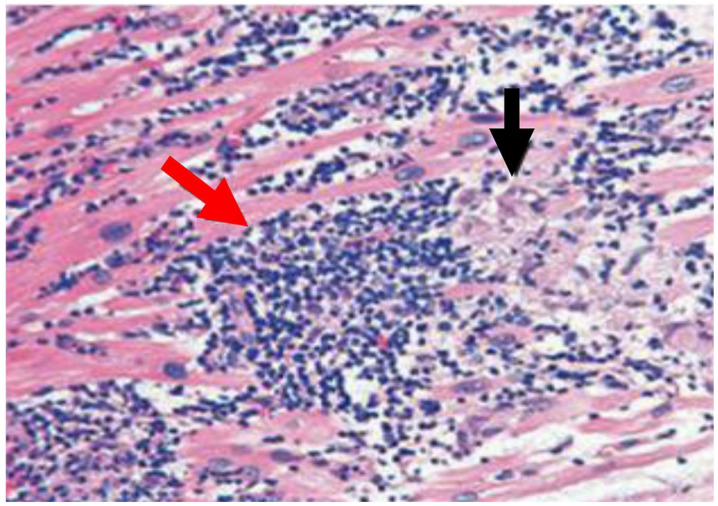
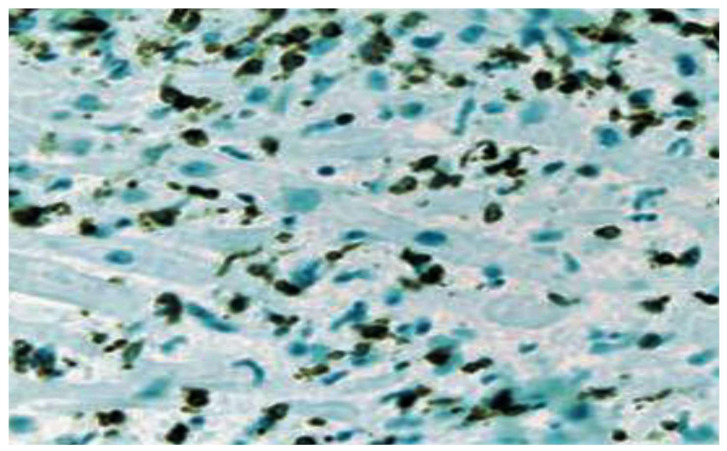
In this review, we investigated whether severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can directly cause myocarditis with severe myocardial damage induced by viral particles. A review of the major data published from 2020 to 2022 was performed by consulting the major databases alongside first-hand experiences that emerged from the cardiac biopsies and autopsy examinations of patients who died of SARS-CoV-2 infections. From this study, a significantly large amount of data suggests that the Dallas criteria were met in a residual percentage of patients, demonstrating that SARS-CoV-2 myocarditis was a rare clinical and pathological entity that occurred in a small percentage of subjects. All cases described here were highly selected and subjected to autopsies or endomyocardial biopsies (EMBs). The most important discovery, through the detection of the SARS-CoV-2 genome using the polymerase chain reaction, consisted in the presence of the viral genome in the lung tissue of most of the patients who died from COVID-19. However, the discovery of the SARS-CoV-2 viral genome was a rare event in cardiac tissue from autopsy findings of patients who died of myocarditis It is important to emphasize that myocardial inflammation alone, as promoted by macrophages and T cell infiltrations, can be observed in noninfectious deaths and COVID-19 cases, but the extent of each cause is varied, and in neither case have such findings been reported to support clinically relevant myocarditis. Therefore, in the different infected vs. non-infected samples examined, none of our findings provide a definitive histochemical assessment for the diagnosis of myocarditis in the majority of cases evaluated. We report evidence suggesting an extremely low frequency of viral myocarditis that has also been associated with unclear therapeutic implications. These two key factors strongly point towards the use of an endomyocardial biopsy to irrefutably reach a diagnosis of viral myocarditis in the context of COVID-19.
Keywords: COVID-19; SARS-CoV-2-induced myocarditis; autopsy; endomyocardial biopsy; myocarditis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Pathological Evidence for SARS-CoV-2 as a Cause of Myocarditis: JACC Review Topic of the Week.J Am Coll Cardiol. 2021 Jan 26;77(3):314-325. doi: 10.1016/j.jacc.2020.11.031. J Am Coll Cardiol. 2021. PMID: 33478655 Free PMC article. Review.
-
Association Between SARS-CoV-2 Infection and Immune-Mediated Myopathy in Patients Who Have Died.JAMA Neurol. 2021 Aug 1;78(8):948-960. doi: 10.1001/jamaneurol.2021.2004. JAMA Neurol. 2021. PMID: 34115106
-
Clinically Suspected Myocarditis in the Course of Severe Acute Respiratory Syndrome Novel Coronavirus-2 Infection: Fact or Fiction?J Card Fail. 2021 Jan;27(1):92-96. doi: 10.1016/j.cardfail.2020.11.002. Epub 2020 Nov 6. J Card Fail. 2021. PMID: 33166657 Free PMC article. Review.
-
Detection of viral SARS-CoV-2 genomes and histopathological changes in endomyocardial biopsies.ESC Heart Fail. 2020 Oct;7(5):2440-2447. doi: 10.1002/ehf2.12805. Epub 2020 Jun 12. ESC Heart Fail. 2020. PMID: 32529795 Free PMC article.
-
Fulminant myocarditis induced by SARS-CoV-2 infection without severe lung involvement: insights into COVID-19 pathogenesis.J Genet Genomics. 2024 Jun;51(6):608-616. doi: 10.1016/j.jgg.2024.02.007. Epub 2024 Mar 4. J Genet Genomics. 2024. PMID: 38447818
Cited by
-
Persistence of SARS-CoV-2 colonization and high expression of inflammatory factors in cardiac tissue 6 months after COVID-19 recovery: a prospective cohort study.Cardiovasc Diagn Ther. 2024 Apr 30;14(2):251-263. doi: 10.21037/cdt-23-381. Epub 2024 Apr 23. Cardiovasc Diagn Ther. 2024. PMID: 38716313 Free PMC article.
-
COVID-19 Detection and Diagnosis Model on CT Scans Based on AI Techniques.Bioengineering (Basel). 2024 Jan 14;11(1):79. doi: 10.3390/bioengineering11010079. Bioengineering (Basel). 2024. PMID: 38247956 Free PMC article.
-
The Impact of Cardiovascular Antecedents on the Prognosis of COVID-19 Critically Ill Patients.J Clin Med. 2024 Jun 15;13(12):3518. doi: 10.3390/jcm13123518. J Clin Med. 2024. PMID: 38930047 Free PMC article.
-
Comparison of left ventricular deformation abnormalities by echocardiography with cardiac magnetic resonance imaging in patients with acute myocarditis and preserved left ventricular ejection fraction.Front Cardiovasc Med. 2024 Jan 9;10:1322145. doi: 10.3389/fcvm.2023.1322145. eCollection 2023. Front Cardiovasc Med. 2024. PMID: 38264261 Free PMC article.
-
Editorial: Unravelling the reality of COVID-19 cardiovascular complications: true myocarditis vs. myocardial injury-the role of a multilayered approach.Front Cardiovasc Med. 2024 Sep 4;11:1481667. doi: 10.3389/fcvm.2024.1481667. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39296377 Free PMC article. No abstract available.
References
-
- Aretz H.T., Billingham M.E., Edwards W.D., Factor S.M., Fallon J.T., Fenoglio J.J., Jr., Olsen E.G., Schoen F.J. Myocarditis. A histopathologic definition and classification. Am. J. Cardiovasc. Pathol. 1987;1:3–14. - PubMed
-
- Strauer B.E. Consensus conference. Myocarditis--dilated cardiomyopathy. Inaugurated by the German Society of Internal Medicine. Internist. 1995;36:484–502. - PubMed
-
- Calabrese F., Angelini A., Carturan E., Thiene G. Ernst Schering Res Found Workshop. Springer; Berlin/Heidelberg, Germany: 2006. Myocarditis and inflammatory cardiomyopathy: Histomorphological diagnosis; pp. 305–321. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
