

Five-Year Sustained Complete Remission With Minimal Adverse Effects Following Radiosurgery for 2-cm Brain Metastasis With Deep Eloquent Location From Lung Adenocarcinoma Despite Low Marginal Dose and High 12 Gy Volume
- PMID: 37113354
- PMCID: PMC10126149
- DOI: 10.7759/cureus.36680
Five-Year Sustained Complete Remission With Minimal Adverse Effects Following Radiosurgery for 2-cm Brain Metastasis With Deep Eloquent Location From Lung Adenocarcinoma Despite Low Marginal Dose and High 12 Gy Volume
Abstract
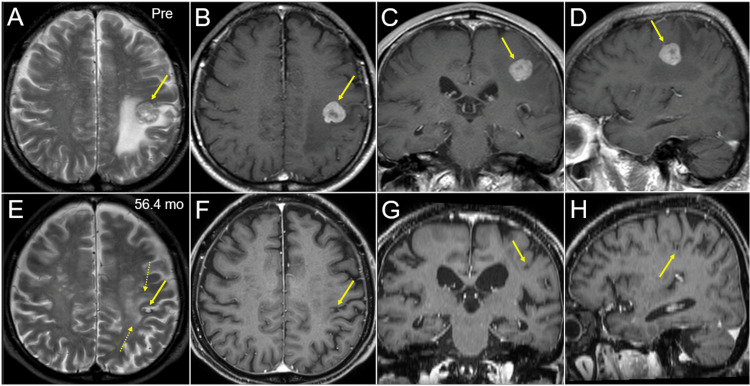
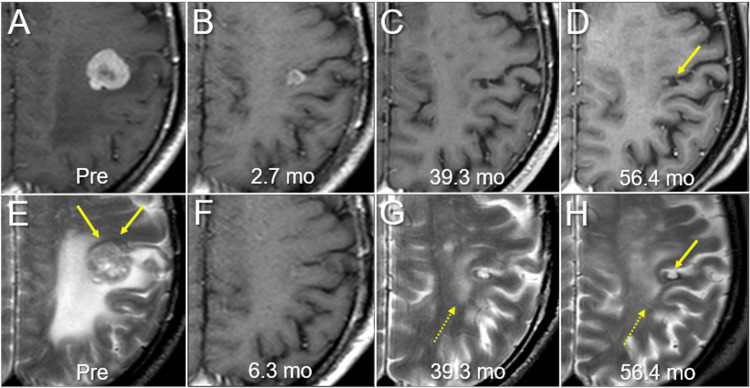
In single-fraction (sf) stereotactic radiosurgery (SRS) for brain metastases (BM) from lung adenocarcinoma (LAC), a marginal dose of ≥22-24 Gy is generally deemed desirable for achieving long-term local tumor control, whereas symptomatic brain radionecrosis significantly increases when the surrounding brain volume receiving ≥12 Gy (V12 Gy) exceeds >5-10 cm3, especially in a deep location. Here, we describe a 75-year-old male with a single LAC-BM of 20 mm in diameter, with a deep eloquent location, which was treated with sfSRS followed by erlotinib, resulting in sustained local complete remission (CR) with minimal adverse radiation effect at nearly five years after sfSRS. The LAC harbored epidermal growth factor receptor (EGFR) mutation. The gross tumor volume (GTV) was defined based on contrast-enhanced computed tomography (CECT) alone. sfSRS was implemented 11 days after planning CECT acquisition. The original GTV had some under- and over-coverage of the enhancing lesion. The D98% values of corrected GTV (cGTV) (3.08 cm3) and 2-mm outside the cGTV were 18.0 Gy with 55% isodose and 14.8 Gy, respectively. The irradiated isodose volumes, including the GTV, receiving ≥22 Gy and ≥12 Gy were 2.18 cm3 and 14.32 cm3, respectively. Erlotinib was administered 13 days after sfSRS with subsequent dose adjustments over 22 months. There was a remarkable tumor response and subsequent nearly CR of the BM were observed at 2.7 and 6.3 months, respectively, with the tumor remnant being visible as a tiny cavitary lesion located in the cortex of the post-central gyrus at 56.4 months. The present case suggests the existence of: (i) extremely radio- and tyrosine kinase inhibitor (TKI)-sensitive LAC-BM for which sfSRS of ≤18 Gy combined with EGFR-TKI is sufficient for attaining long-term CR; and (ii) long-term brain tolerance following sfSRS despite high 12 Gy volume and deep eloquent location in the late 70s The moderate marginal dose of the GTV, the main location of the BM in the cerebral cortex, and the excellent tumor responses with sufficient extrication from the mass effect may render the BM immune to late adverse radiation effect.
Keywords: brain metastasis; brain radionecrosis; dose distribution; dose gradient; lung adenocarcinoma; non-small cell lung cancer; radiotherapy treatment planning; single fraction stereotactic radiosurgery; tyrosine kinase inhibitor; volumetric modulated arc therapy.
Copyright © 2023, Ohtakara et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- The impact of EGFR-TKI use on clinical outcomes of lung adenocarcinoma patients with brain metastases after Gamma Knife radiosurgery: a propensity score-matched analysis based on extended JLGK0901 dataset (JLGK0901-EGFR-TKI) Yomo S, Serizawa T, Yamamoto M, et al. J Neurooncol. 2019;145:151–157. - PubMed
-
- Management of brain metastases in tyrosine kinase inhibitor-naïve epidermal growth factor receptor-mutant non-small-cell lung cancer: a retrospective multi-institutional analysis. Magnuson WJ, Lester-Coll NH, Wu AJ, et al. J Clin Oncol. 2017;35:1070–1077. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous