

Inappropriate Shock Delivery Is Common During Pediatric In-Hospital Cardiac Arrest
- PMID: 37115167
- PMCID: PMC10440232
- DOI: 10.1097/PCC.0000000000003241
Inappropriate Shock Delivery Is Common During Pediatric In-Hospital Cardiac Arrest
Abstract
Objectives: To characterize inappropriate shock delivery during pediatric in-hospital cardiac arrest (IHCA).
Design: Retrospective cohort study.
Setting: An international pediatric cardiac arrest quality improvement collaborative Pediatric Resuscitation Quality [pediRES-Q].
Patients: All IHCA events from 2015 to 2020 from the pediRES-Q Collaborative for which shock and electrocardiogram waveform data were available.
Interventions: None.
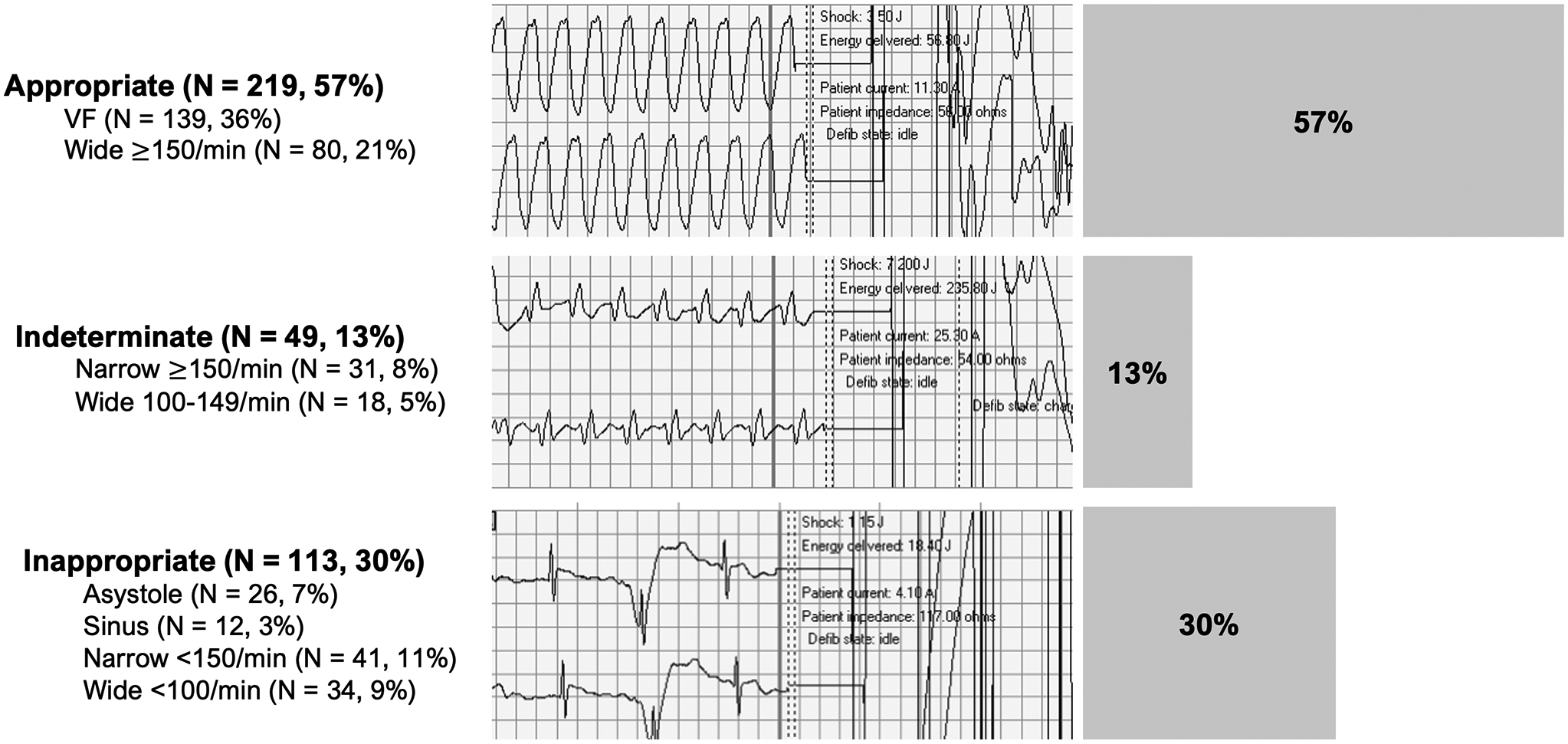
Measurements and main results: We analyzed 418 shocks delivered during 159 cardiac arrest events, with 381 shocks during 158 events at 28 sites remaining after excluding undecipherable rhythms. We classified shocks as: 1) appropriate (ventricular fibrillation [VF] or wide complex ≥ 150/min); 2) indeterminate (narrow complex ≥ 150/min or wide complex 100-149/min); or 3) inappropriate (asystole, sinus, narrow complex < 150/min, or wide complex < 100/min) based on the rhythm immediately preceding shock delivery. Of delivered shocks, 57% were delivered appropriately for VF or wide complex rhythms with a rate greater than or equal to 150/min. Thirteen percent were classified as indeterminate. Thirty percent were delivered inappropriately for asystole (6.8%), sinus (3.1%), narrow complex less than 150/min (11%), or wide complex less than 100/min (8.9%) rhythms. Eighty-eight percent of all shocks were delivered in ICUs or emergency departments, and 30% of those were delivered inappropriately.
Conclusions: The rate of inappropriate shock delivery for pediatric IHCA in this international cohort is at least 30%, with 23% delivered to an organized electrical rhythm, identifying opportunity for improvement in rhythm identification training.
Trial registration: ClinicalTrials.gov NCT02708134.
Copyright © 2023 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Drs. Gray’s, Tegmeyer’s, Nadkarni’s, and Dewan’s institutions received funding from ZOLL Medical. Dr. Atkins received funding from the National Institutes of Health (NIH) and the Pediatric Heart Network. Dr. Nadkarni’s institution received funding from the Laerdal Foundation and RQI Partners; he received funding from the Society of Critical Care Medicine as the President-Elect 2023–2024. Niles and Dr. Nadkarni disclosed that The Children’s Hospital of Philadelphia receives support from an unrestricted research grant from ZOLL Medical (Chelmsford, MA). Ms. Niles and Dr. Nadkarni disclose that The Children’s Hospital of Philadelphia receives funding from an unrestricted research grant from The American Heart Association (Chicago, IL). Dr. Pandit disclosed that he is an employee of ZOLL Medical. Dr. Dewan received support for article research from the NIH. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Samson RA, Nadkarni VM, Meaney PA, et al.: Outcomes of In-Hospital Ventricular Fibrillation in Children. The New England Journal of Medicine 2006; 354:2328–39 - PubMed
-
- Topjian AA, Raymond TT, Atkins D, et al.: Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020; 142:S469–S523 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
