

Global dietary quality in 185 countries from 1990 to 2018 show wide differences by nation, age, education, and urbanicity
- PMID: 37118151
- PMCID: PMC10277807
- DOI: 10.1038/s43016-022-00594-9
Global dietary quality in 185 countries from 1990 to 2018 show wide differences by nation, age, education, and urbanicity
Abstract
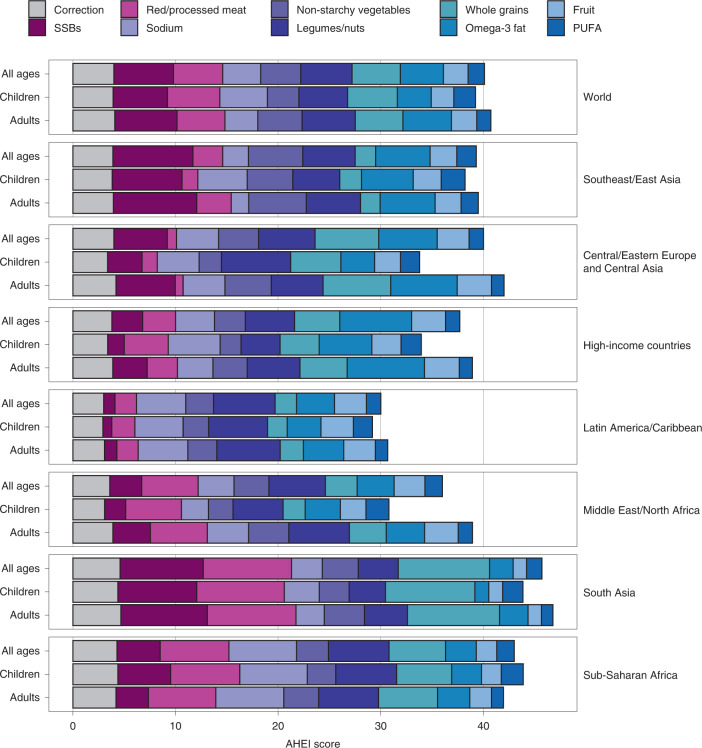
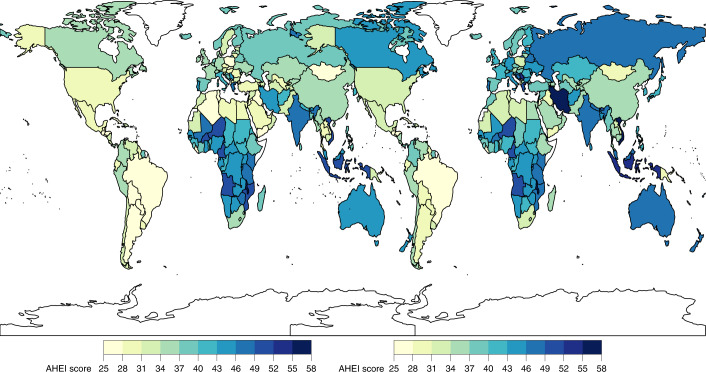
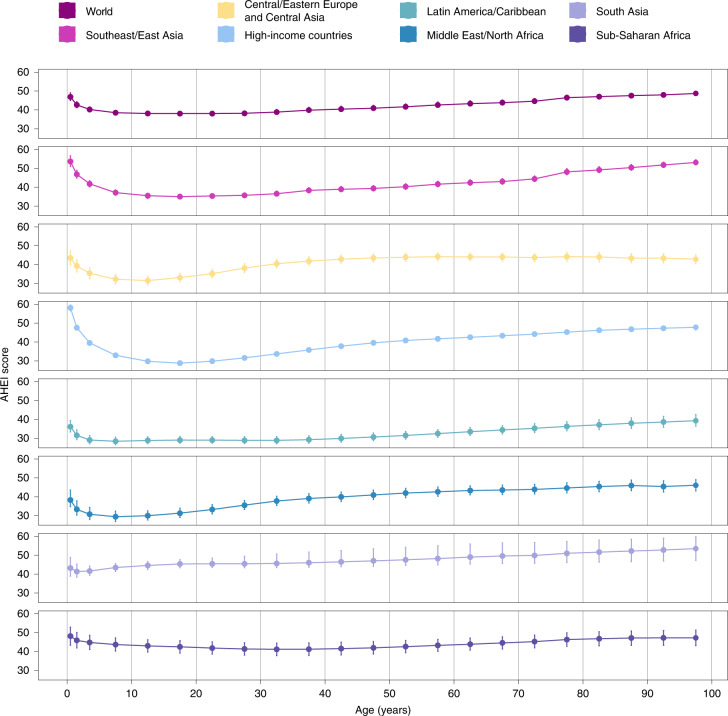
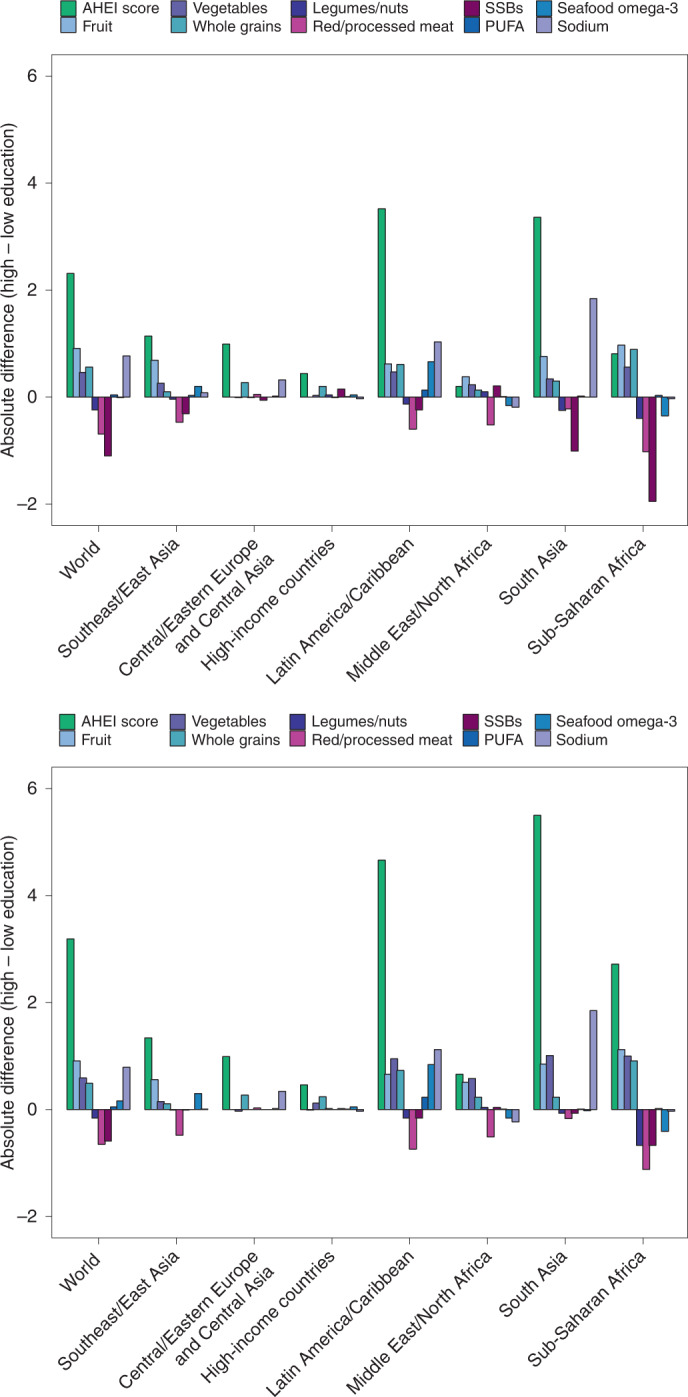
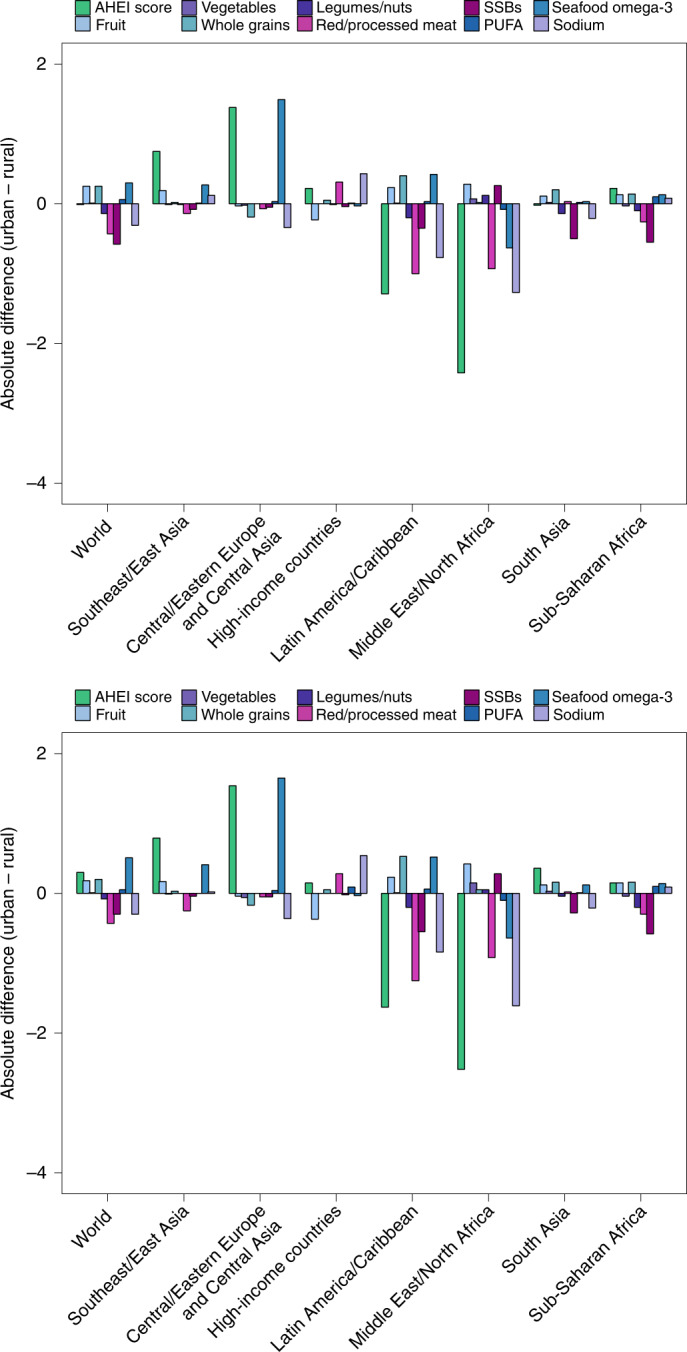
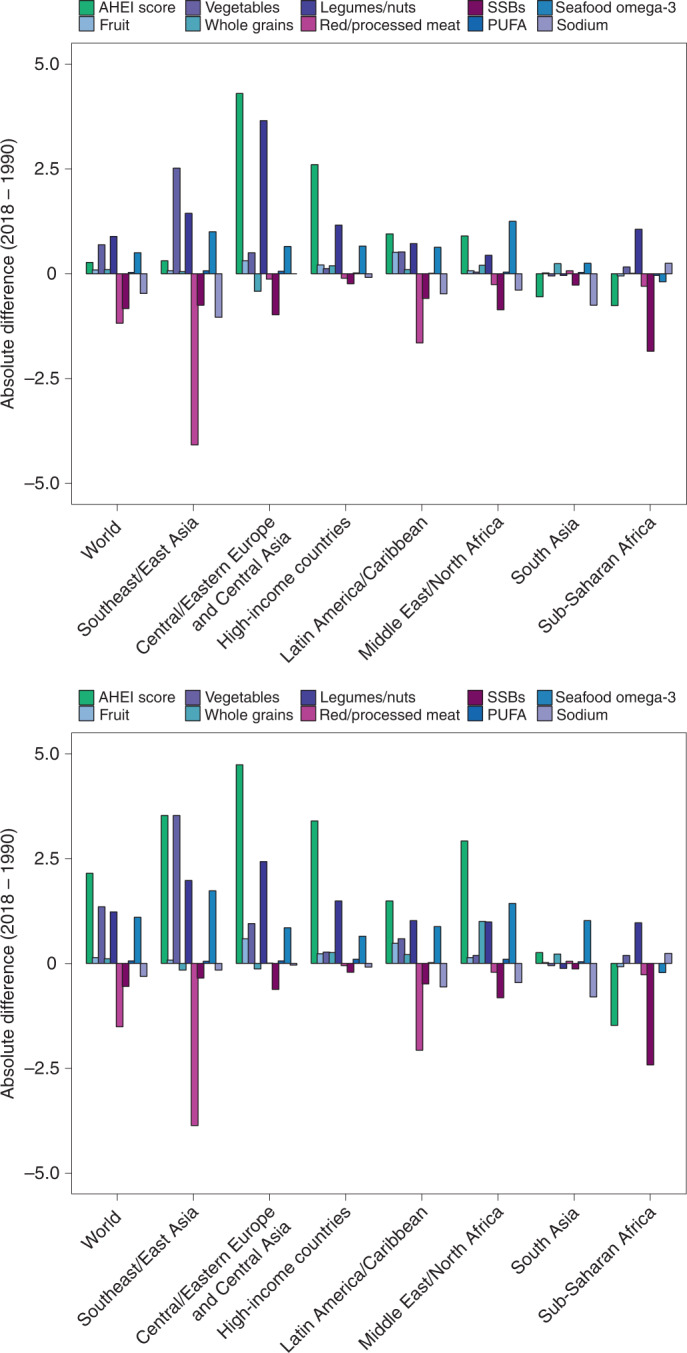
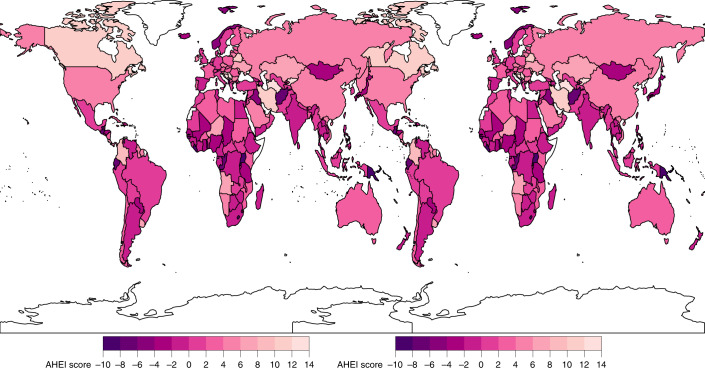
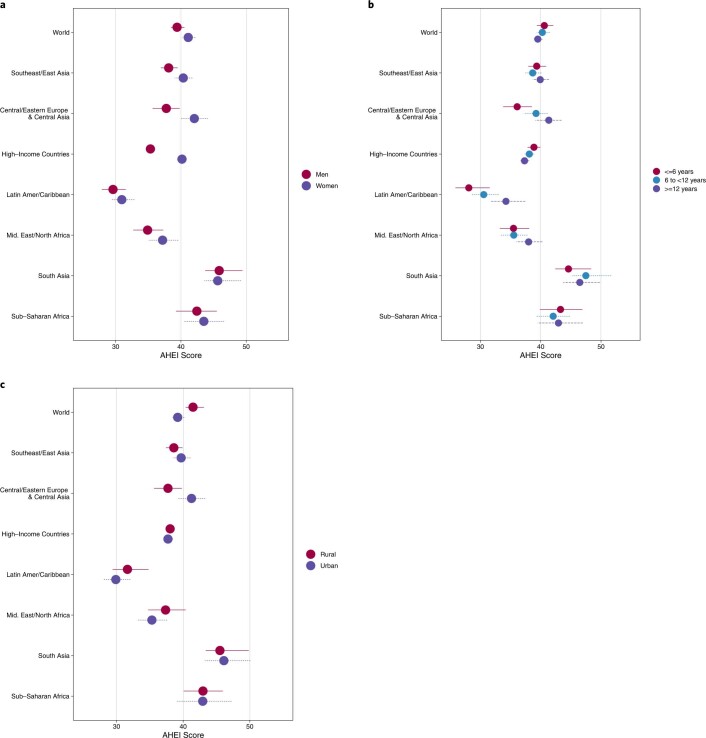
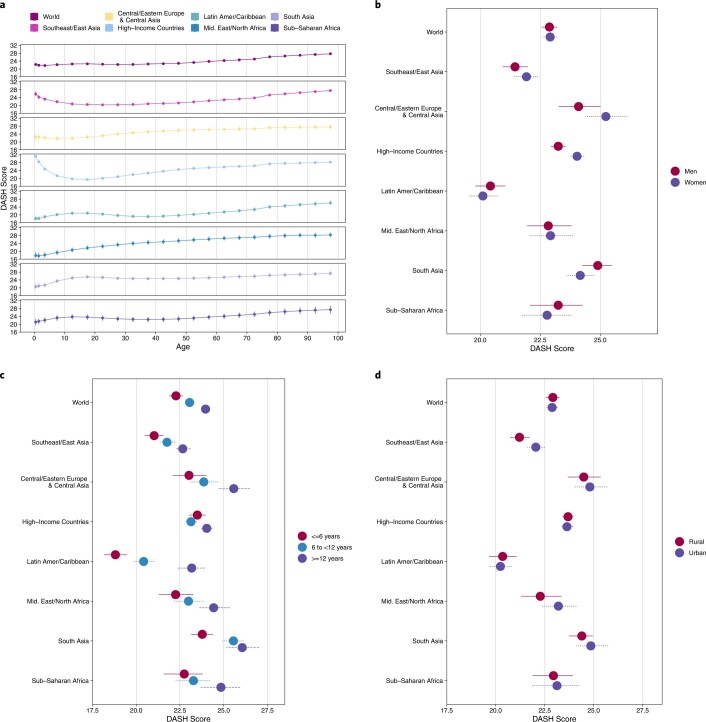
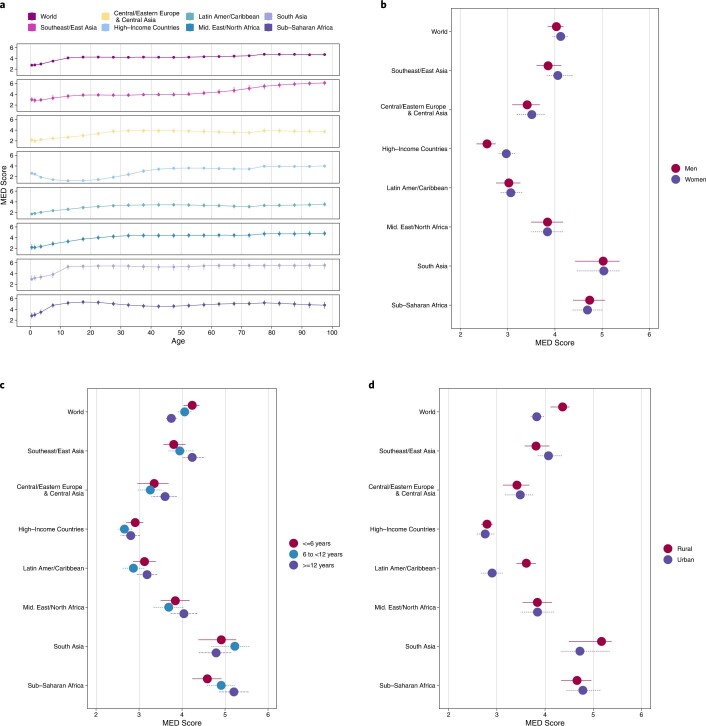
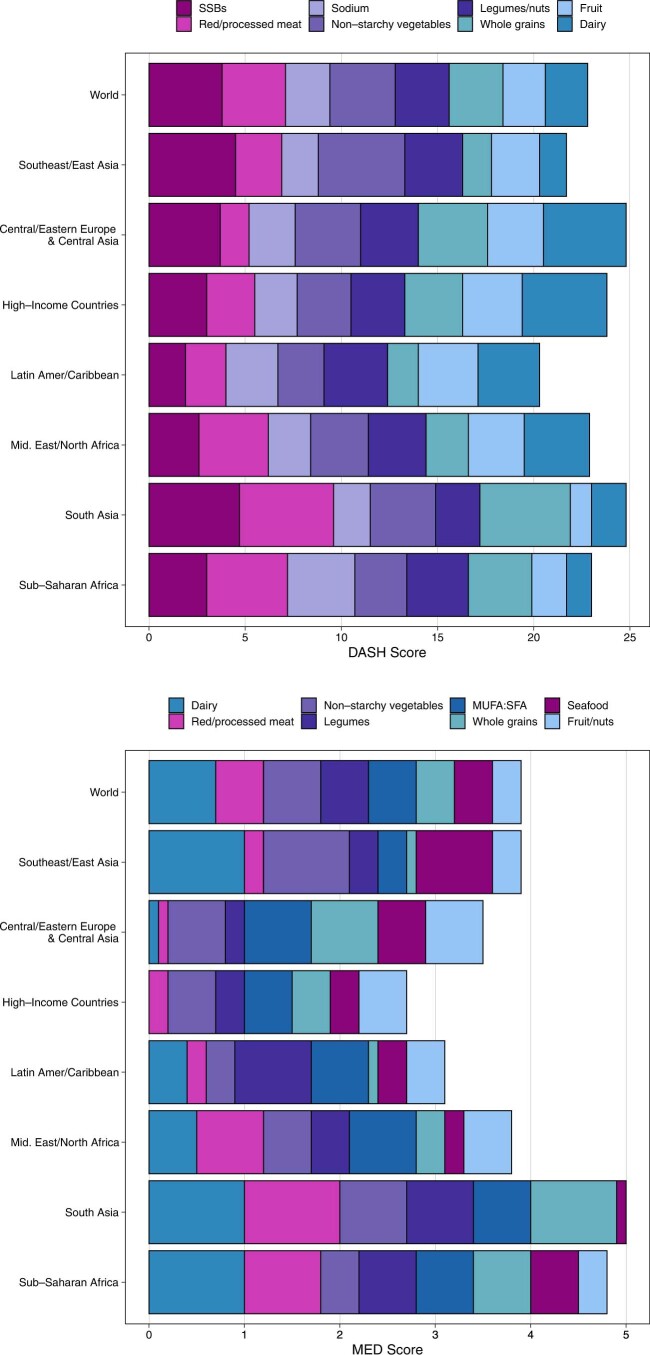
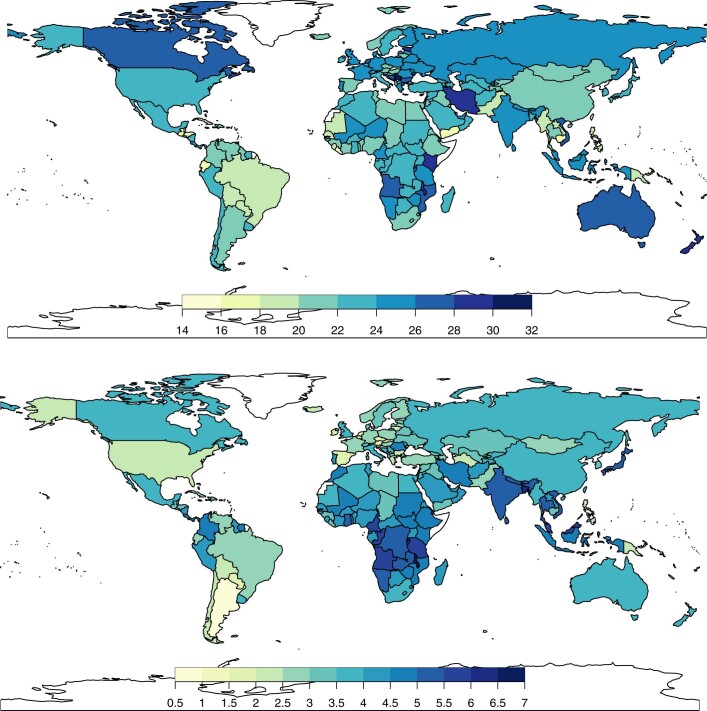
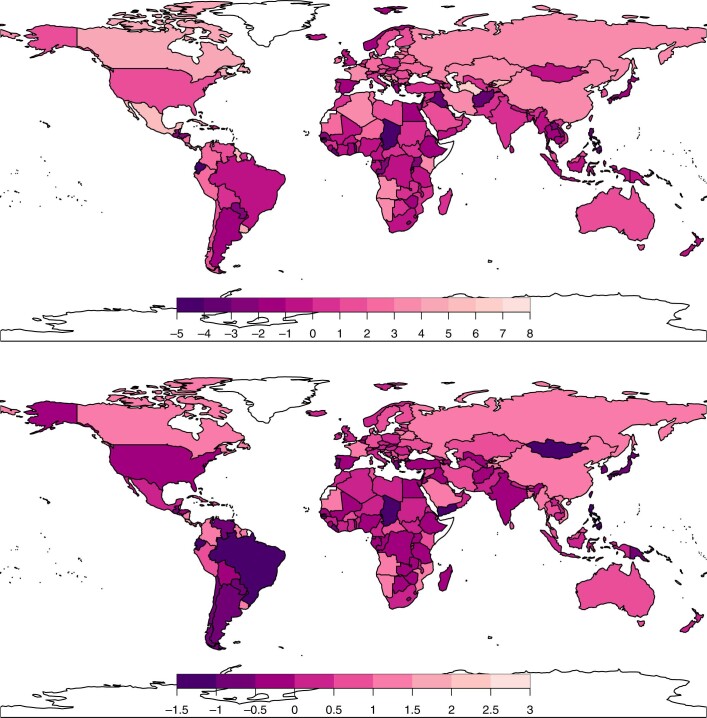
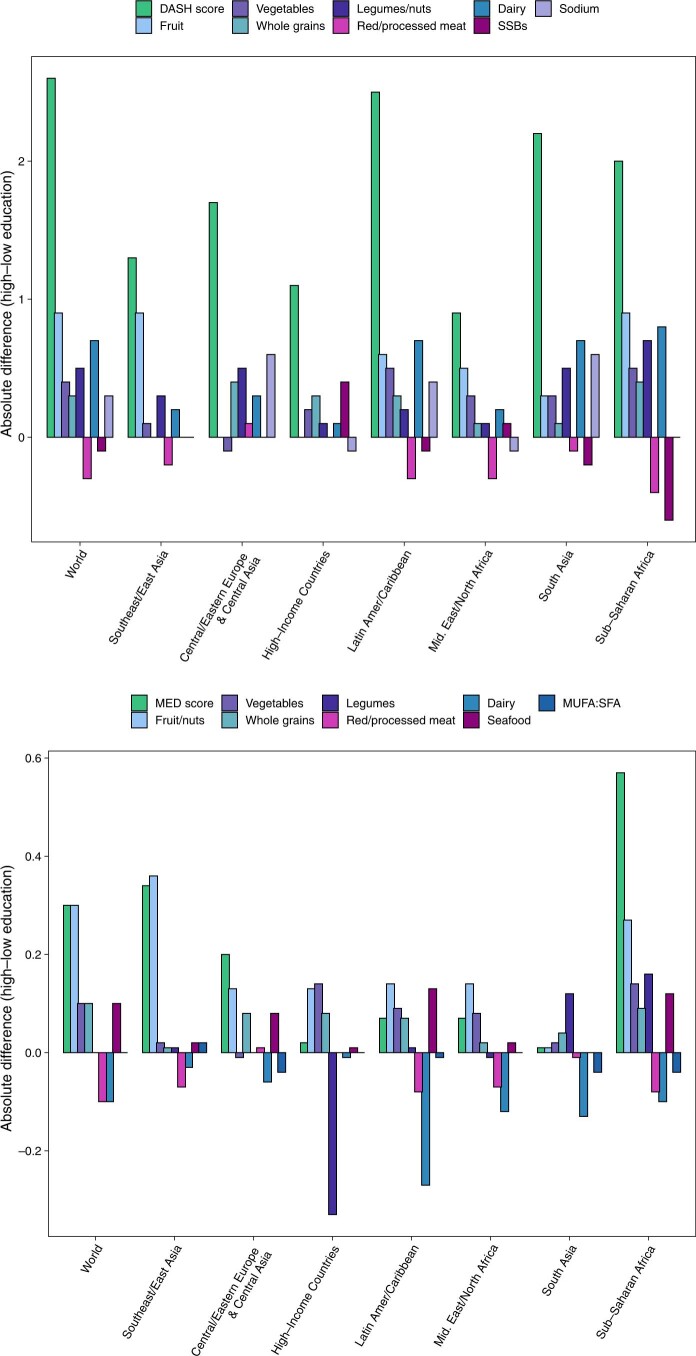
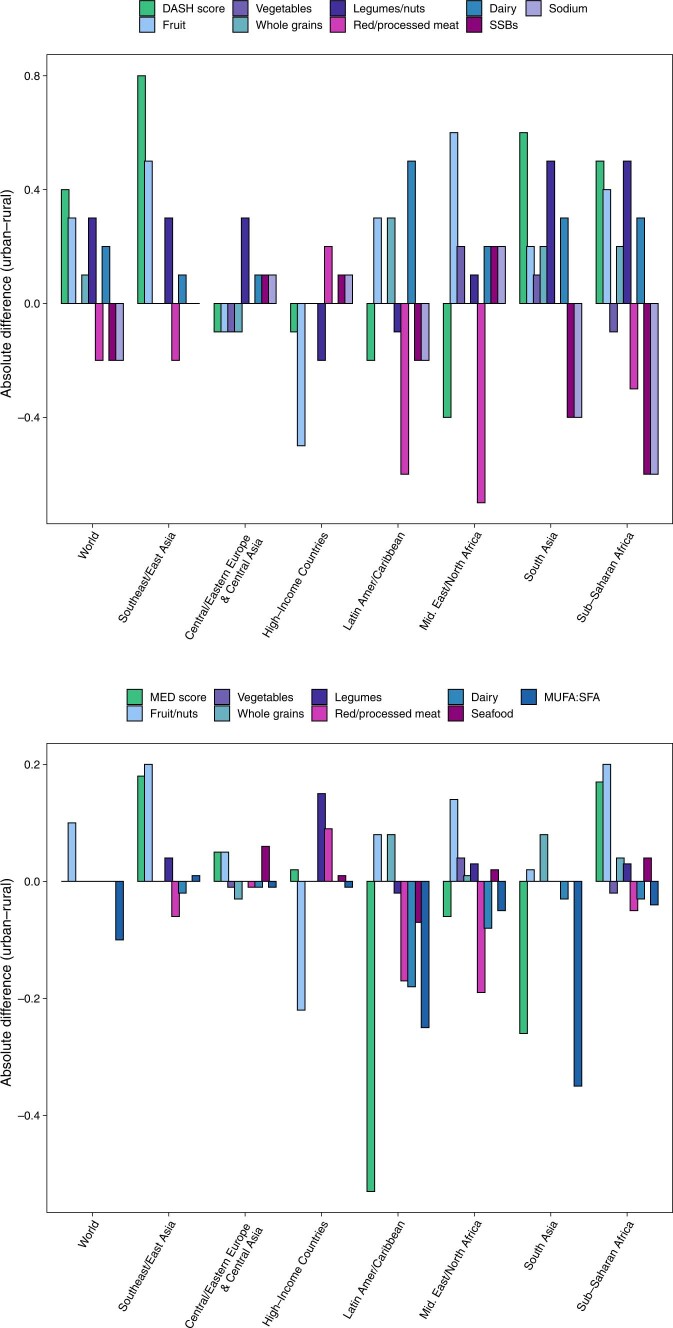
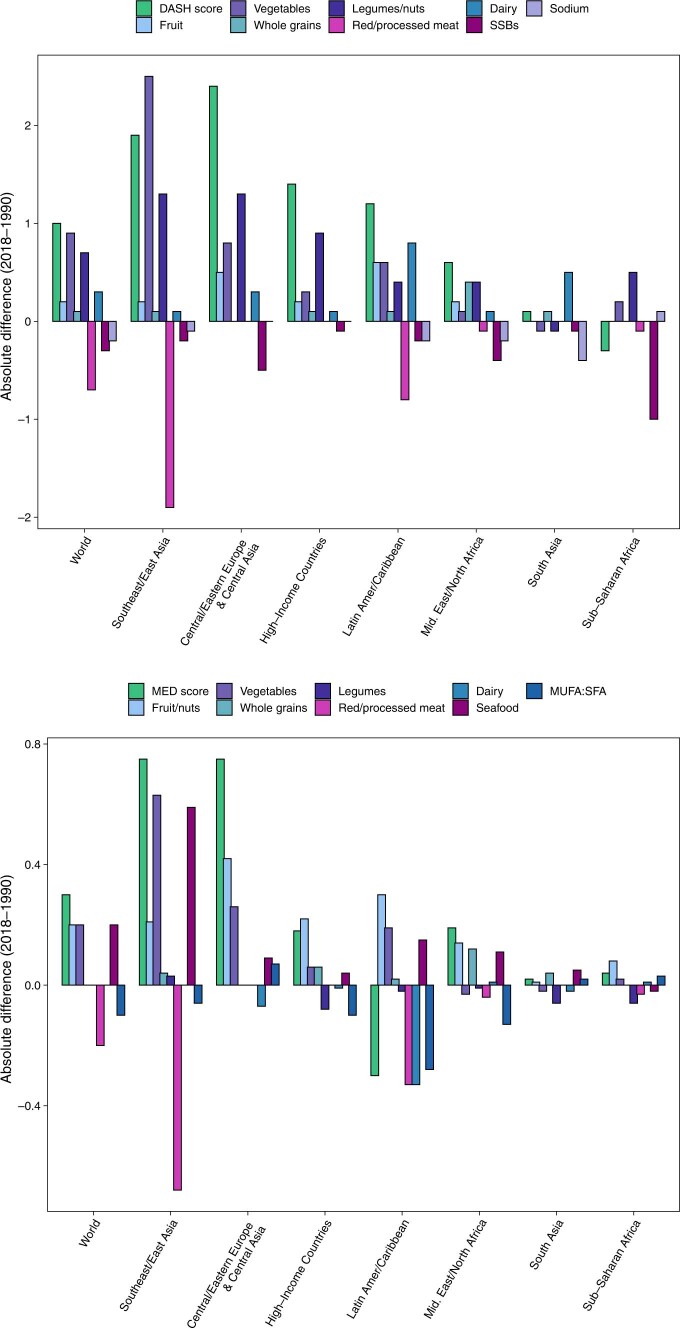
Evidence on what people eat globally is limited in scope and rigour, especially as it relates to children and adolescents. This impairs target setting and investment in evidence-based actions to support healthy sustainable diets. Here we quantified global, regional and national dietary patterns among children and adults, by age group, sex, education and urbanicity, across 185 countries between 1990 and 2018, on the basis of data from the Global Dietary Database project. Our primary measure was the Alternative Healthy Eating Index, a validated score of diet quality; Dietary Approaches to Stop Hypertension and Mediterranean Diet Score patterns were secondarily assessed. Dietary quality is generally modest worldwide. In 2018, the mean global Alternative Healthy Eating Index score was 40.3, ranging from 0 (least healthy) to 100 (most healthy), with regional means ranging from 30.3 in Latin America and the Caribbean to 45.7 in South Asia. Scores among children versus adults were generally similar across regions, except in Central/Eastern Europe and Central Asia, high-income countries, and the Middle East and Northern Africa, where children had lower diet quality. Globally, diet quality scores were higher among women versus men, and more versus less educated individuals. Diet quality increased modestly between 1990 and 2018 globally and in all world regions except in South Asia and Sub-Saharan Africa, where it did not improve.
© 2022. The Author(s).
Conflict of interest statement
V.M. reports research funding from the Canadian Institutes of Health Research, outside the submitted work. P.W. reports research grants and contracts from the United States Agency for International Development and personal fees from the Global Panel on Agriculture and Food Systems for Nutrition, outside the submitted work. J.R., J.Z. and P.S. report research funding from Nestlé, outside the submitted work. J.C. reports research funding from the Bill and Melinda Gates Foundation and the United States Agency for International Development, and personal fees from UNICEF/WHO, outside the submitted work. D.M. reports research funding from the National Institutes of Health and the Bill and Melinda Gates Foundation; personal fees from GOED, Bunge, Indigo Agriculture, Motif FoodWorks, Amarin, Acasti Pharma, Cleveland Clinic Foundation, America’s Test Kitchen and Danone; scientific advisory board member for Brightseed, DayTwo, Elysium Health, Filtricine, HumanCo and Tiny Organics; and chapter royalties from UpToDate, all outside the submitted work. The other authors have no disclosures to declare.
Figures
References
-
- 2021 Global Nutrition Report: The State of Global Nutrition (Development Initiatives, 2021).
-
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet10.1016/s0140-6736(18)32225-6 (2018). - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
