

Strong peak immunogenicity but rapid antibody waning following third vaccine dose in older residents of care homes
- PMID: 37118525
- PMCID: PMC10154221
- DOI: 10.1038/s43587-022-00328-3
Strong peak immunogenicity but rapid antibody waning following third vaccine dose in older residents of care homes
Abstract
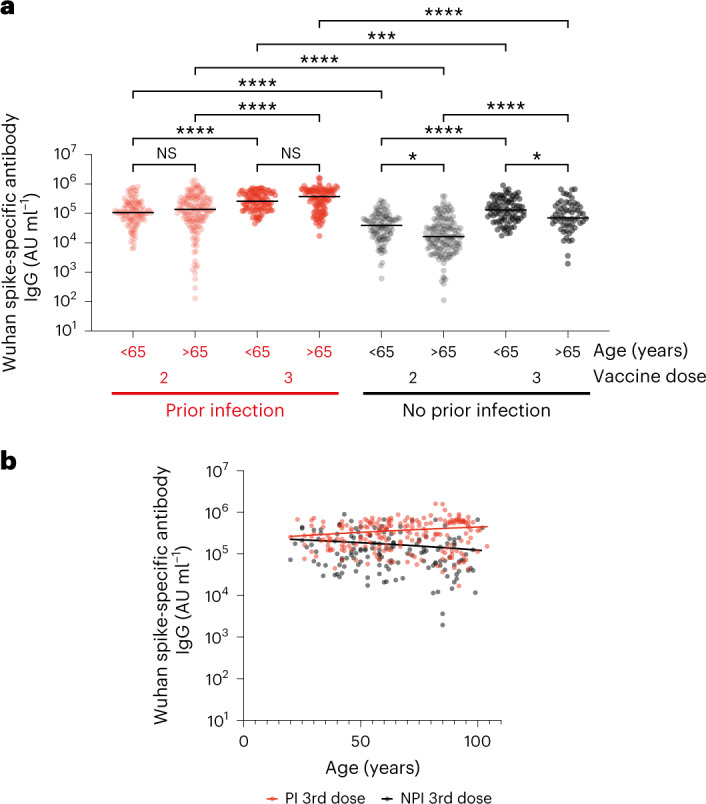
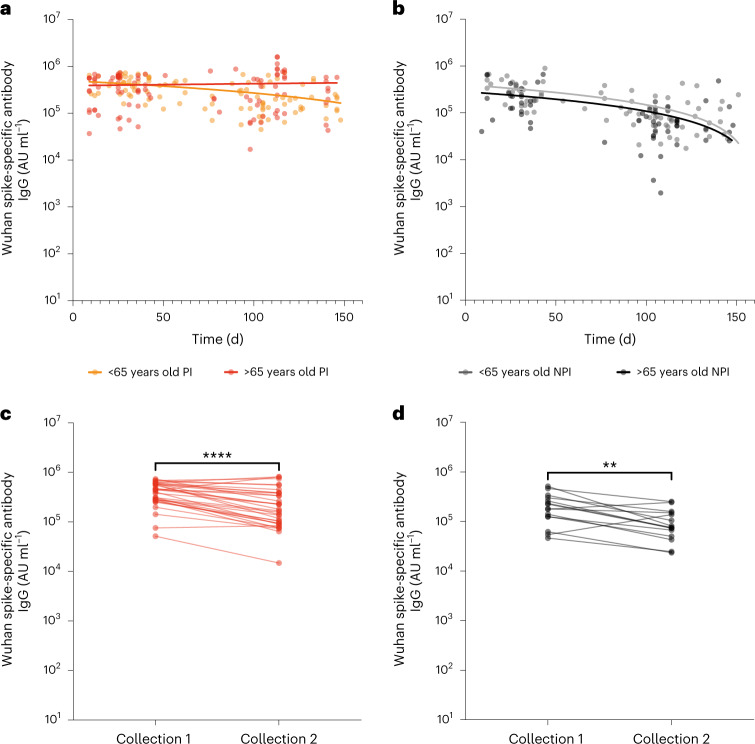
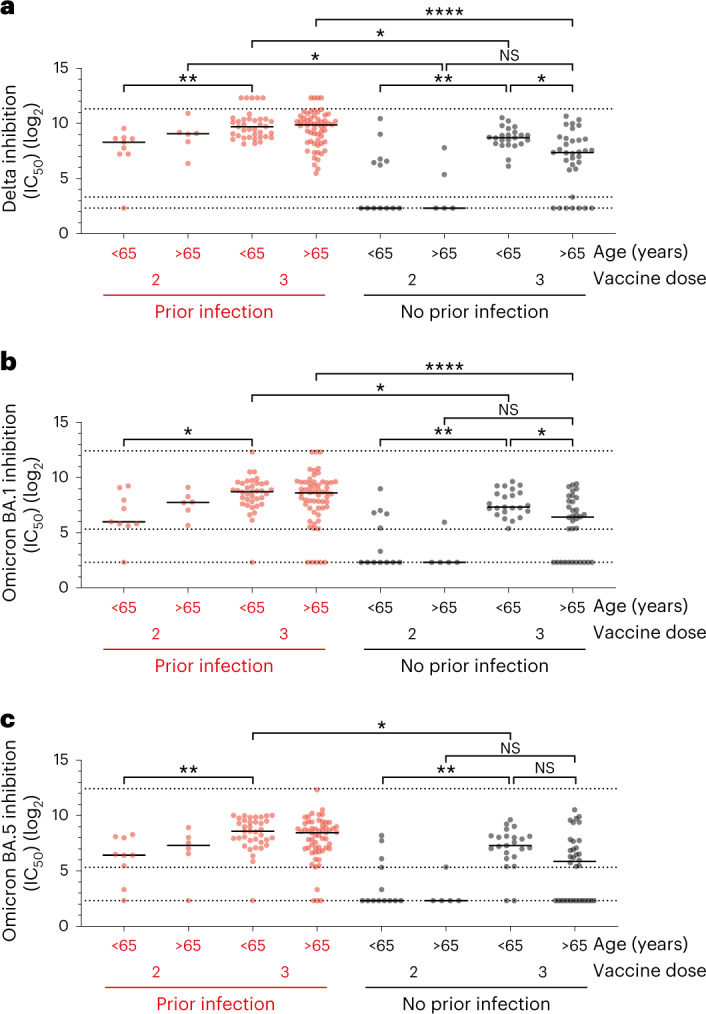
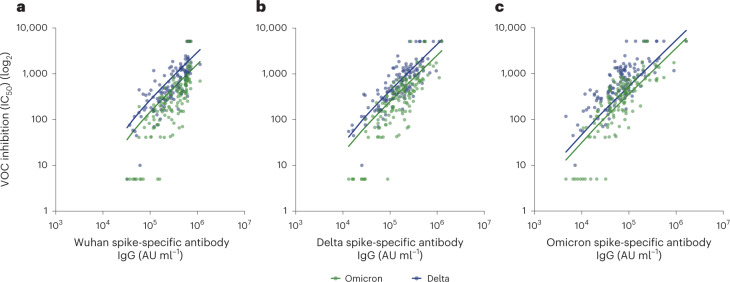
Third-dose coronavirus disease 2019 vaccines are being deployed widely but their efficacy has not been assessed adequately in vulnerable older people who exhibit suboptimal responses after primary vaccination series. This observational study, which was carried out by the VIVALDI study based in England, looked at spike-specific immune responses in 341 staff and residents in long-term care facilities who received an mRNA vaccine following dual primary series vaccination with BNT162b2 or ChAdOx1. Third-dose vaccination strongly increased antibody responses with preferential relative enhancement in older people and was required to elicit neutralization of Omicron. Cellular immune responses were also enhanced with strong cross-reactive recognition of Omicron. However, antibody titers fell 21-78% within 100 d after vaccine and 27% of participants developed a breakthrough Omicron infection. These findings reveal strong immunogenicity of a third vaccine in one of the most vulnerable population groups and endorse an approach for widespread delivery across this population. Ongoing assessment will be required to determine the stability of immune protection.
© 2023. The Author(s).
Conflict of interest statement
L.S. reports grants from the Department of Health and Social Care during the conduct of the study and is a member of the Social Care Working Group, which reports to the Scientific Advisory Group for Emergencies. A.H. is a member of the New and Emerging Respiratory Virus Threats Advisory Group at the Department of Health. The remaining authors declare no competing interests.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
