

Intersurgeon Variability in Local Treatment Planning for Patients with Initially Unresectable Colorectal Cancer Liver Metastases: Analysis of the Liver Expert Panel of the Dutch Colorectal Cancer Group
- PMID: 37118612
- PMCID: PMC10409679
- DOI: 10.1245/s10434-023-13510-7
Intersurgeon Variability in Local Treatment Planning for Patients with Initially Unresectable Colorectal Cancer Liver Metastases: Analysis of the Liver Expert Panel of the Dutch Colorectal Cancer Group
Abstract
Background: Consensus on resectability criteria for colorectal cancer liver metastases (CRLM) is lacking, resulting in differences in therapeutic strategies. This study evaluated variability of resectability assessments and local treatment plans for patients with initially unresectable CRLM by the liver expert panel from the randomised phase III CAIRO5 study.
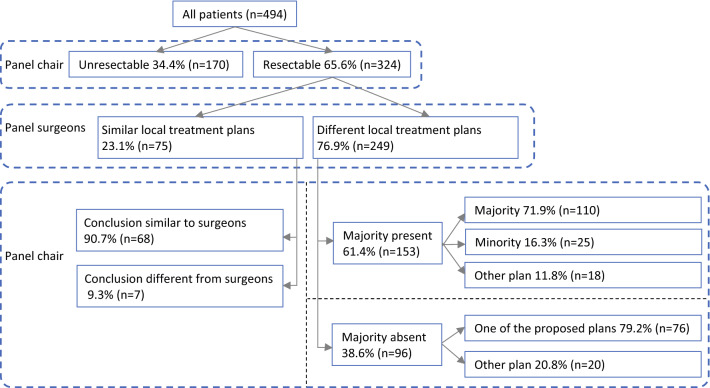
Methods: The liver panel, comprising surgeons and radiologists, evaluated resectability by predefined criteria at baseline and 2-monthly thereafter. If surgeons judged CRLM as resectable, detailed local treatment plans were provided. The panel chair determined the conclusion of resectability status and local treatment advice, and forwarded it to local surgeons.
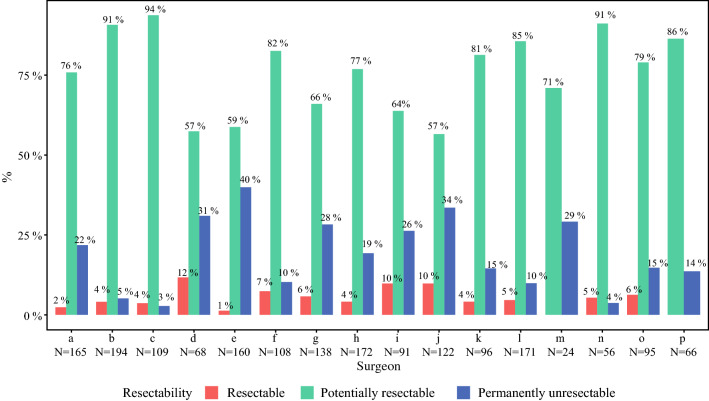
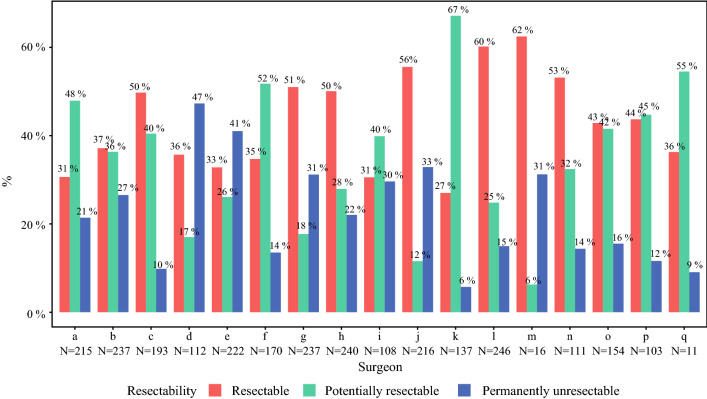
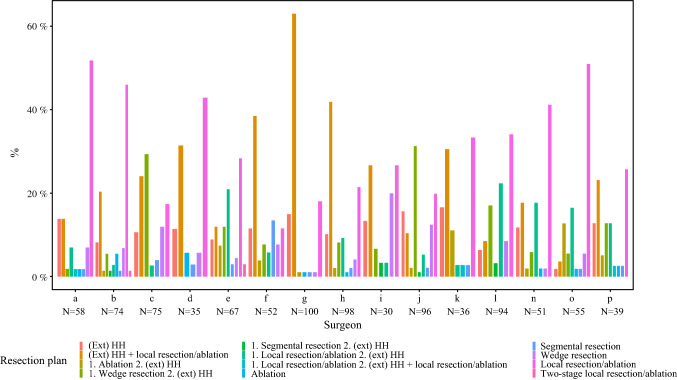
Results: A total of 1149 panel evaluations of 496 patients were included. Intersurgeon disagreement was observed in 50% of evaluations and was lower at baseline than follow-up (36% vs. 60%, p < 0.001). Among surgeons in general, votes for resectable CRLM at baseline and follow-up ranged between 0-12% and 27-62%, and for permanently unresectable CRLM between 3-40% and 6-47%, respectively. Surgeons proposed different local treatment plans in 77% of patients. The most pronounced intersurgeon differences concerned the advice to proceed with hemihepatectomy versus parenchymal-preserving approaches. Eighty-four percent of patients judged by the panel as having resectable CRLM indeed received local treatment. Local surgeons followed the technical plan proposed by the panel in 40% of patients.
Conclusion: Considerable variability exists among expert liver surgeons in assessing resectability and local treatment planning of initially unresectable CRLM. This stresses the value of panel-based decisions, and the need for consensus guidelines on resectability criteria and technical approach to prevent unwarranted variability in clinical practice.
© 2023. The Author(s).
Conflict of interest statement
C.J.A.P. has an advisory role for Nordic Pharma. K.B. reports having an advisory role for Amgen. J.H.W.d.W. has an unrestricted grant from Medtronic. U.P.N. reports presentations or contribution to research for Roche, Astra Zeneca, Merck AG, Sanofi, Grünenthal, Johnson & Johnson and Astellas. This funding is not related to the current research. The remaining authors declare no potential conflicts of interest.
Figures
Comment in
-
ASO Author Reflections: Towards Consensus on Resectability Assessments and Local Treatment Planning for Patients with Initially Unresectable Colorectal Cancer Liver Metastases.Ann Surg Oncol. 2023 Sep;30(9):5386-5387. doi: 10.1245/s10434-023-13513-4. Epub 2023 Apr 21. Ann Surg Oncol. 2023. PMID: 37085656 Free PMC article. No abstract available.
References
-
- Lam VWT, Spiro C, Laurence JM, et al. A systematic review of clinical response and survival outcomes of downsizing systemic chemotherapy and rescue liver surgery in patients with initially unresectable colorectal liver metastases. Ann Surg Oncol. 2012;19(4):1292–1301. doi: 10.1245/s10434-011-2061-0. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
