

Effects of Dapagliflozin in Chronic Kidney Disease, With and Without Other Cardiovascular Medications: DAPA-CKD Trial
- PMID: 37119064
- PMCID: PMC10227210
- DOI: 10.1161/JAHA.122.028739
Effects of Dapagliflozin in Chronic Kidney Disease, With and Without Other Cardiovascular Medications: DAPA-CKD Trial
Abstract
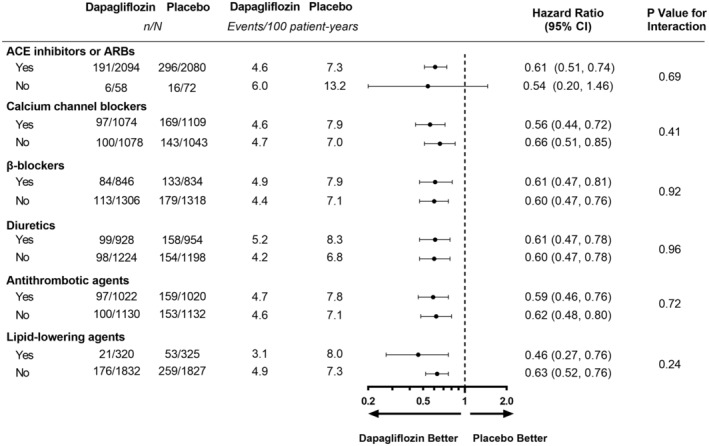
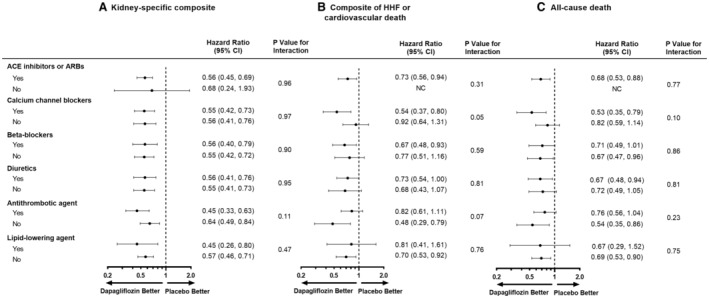
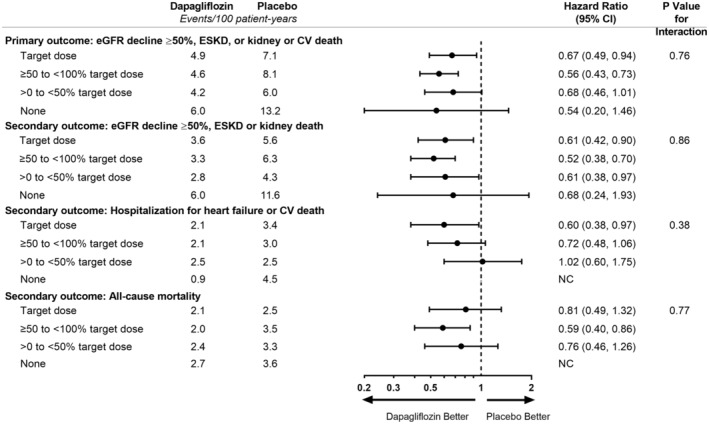
Background The DAPA-CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) trial (NCT03036150) demonstrated that dapagliflozin reduced the risk of kidney and cardiovascular events in patients with chronic kidney disease and albuminuria with and without type 2 diabetes. We aimed to determine whether baseline cardiovascular medication use modified the dapagliflozin treatment effect. Methods and Results We randomized 4304 adults with baseline estimated glomerular filtration rate 25 to 75 mL/min per 1.73 m2 and urinary albumin:creatinine ratio 200 to 5000 mg/g to dapagliflozin 10 mg or placebo once daily. The primary end point was a composite of ≥50% estimated glomerular filtration rate decline, end-stage kidney disease, and kidney or cardiovascular death. Secondary end points included a kidney composite end point (primary composite end point without cardiovascular death), a cardiovascular composite end point (hospitalized heart failure or cardiovascular death), and all-cause mortality. We categorized patients according to baseline cardiovascular medication use/nonuse. Patients were required by protocol to receive a stable (and maximally tolerated) dose of a renin-angiotensin-aldosterone system inhibitor. We observed consistent benefits of dapagliflozin relative to placebo, irrespective of baseline use/nonuse of renin-angiotensin-aldosterone system inhibitors (98.1%), calcium channel blockers (50.7%), β-adrenergic antagonists (39.0%), diuretics (43.7%), and antithrombotic (47.4%), and lipid-lowering (15.0%) agents. Use of these drugs in combination with dapagliflozin did not increase the number of serious adverse events. Conclusions The safety profile and efficacy of dapagliflozin on kidney and cardiovascular end points in patients with chronic kidney disease were consistent among patients treated and not treated at baseline with a range of cardiovascular medications. Registration Information clinicaltrials.gov. Identifier: NCT03036150.
Keywords: SGLT2 inhibitors; cardiovascular medications; chronic kidney disease; dapagliflozin.
Figures
References
-
- Wheeler DC, Stefansson BV, Batiushin M, Bilchenko O, Cherney DZI, Chertow GM, Douthat W, Dwyer JP, Escudero E, Pecoits‐Filho R, et al. The dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA‐CKD) trial: baseline characteristics. Nephrol Dial Transplant. 2020;35:1700–1711. doi: 10.1093/ndt/gfaa234 - DOI - PMC - PubMed
-
- McMurray JJV, Wheeler DC, Stefánsson BV, Jongs N, Postmus D, Correa‐Rotter R, Chertow GM, Greene T, Held C, Hou FF, et al. Effect of dapagliflozin on clinical outcomes in patients with chronic kidney disease, with and without cardiovascular disease. Circulation. 2021;143:438–448. doi: 10.1161/CIRCULATIONAHA.120.051675 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
