

Type II pleuropulmonary blastoma mistaken for rhabdomyosarcoma: A case report
- PMID: 37119756
- PMCID: PMC10163632
- DOI: 10.1016/j.ijscr.2023.108261
Type II pleuropulmonary blastoma mistaken for rhabdomyosarcoma: A case report
Abstract
Introduction: Pleuropulmonary blastoma (PPB) is rare, representing 0.3 % of all pediatric cancers. PPB is classified into three subtypes and may progress from type I to types II and III, with a worse prognosis. Given its rarity, the diagnosis is frequently challenging.
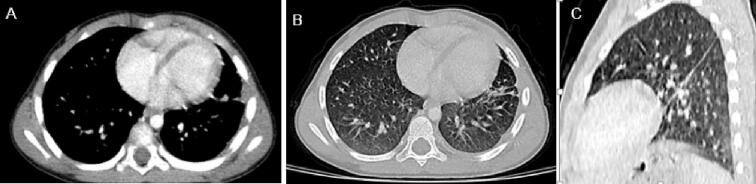
Case presentation: We report an occurrence of PPB in a 3-year-old girl, who presented recurrent pneumopathy. Imaging investigations revealed a large solid lesion in the left hemithorax. Biopsy followed by histological analysis suggested rhabdomyosarcoma. The patient received neoadjuvant chemotherapy before proceeding to complete tumor excision. Surgical exploration revealed that the tumor was primitively related to parietal pleura and lower lobe of left lung. Histopathology of the tumor retained a definitive diagnosis of PPB type II. Postoperative course was uneventful, and a cerebral MRI ruled out brain metastasis. Adjuvant chemotherapy was administered.
Discussion: Clinical expression of PPB is nonspecific and variable. It ranges from a dry cough to respiratory distress. Standard radiography is the first examination to perform and CT is the gold standard for characterization thoracic masses. Surgery and chemotherapy are the pillars of treatment. Indications depend on the tumor type, its extent and its resectability.
Conclusion: PPB is an aggressive tumor that occurs only in children. Due to the rarity of PPB, evidence on optimal treatment is still insufficient. Careful follow-up is necessary searching for local recurrence or metastasis.
Keywords: Case report; Pediatric neoplasms; Pleuropulmonary blastoma; Pneumoblastoma; Rhabdomyosarcoma; Thoracic neoplasm.
Copyright © 2023. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of competing interest The authors declare that there are no conflicts of interest regarding the publication of this article.
Figures




References
-
- Dehner L.P. Pleuropulmonary blastoma is THE pulmonary blastoma of childhood. Semin. Diagn. Pathol. 1994;11(2):144–151. - PubMed
-
- Agha R.A., Franchi T., Sohrab C., Mathew G., Kirwan A., Thomas A., et al. The SCARE 2020 guideline: updating consensus surgical case report (SCARE) guidelines. Int. J. Surg. 2020;84(1):226–230. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
