

A coordinated approach for managing polypharmacy among children with medical complexity: rationale and design of the Pediatric Medication Therapy Management (pMTM) randomized controlled trial
- PMID: 37120509
- PMCID: PMC10148507
- DOI: 10.1186/s12913-023-09439-y
A coordinated approach for managing polypharmacy among children with medical complexity: rationale and design of the Pediatric Medication Therapy Management (pMTM) randomized controlled trial
Abstract
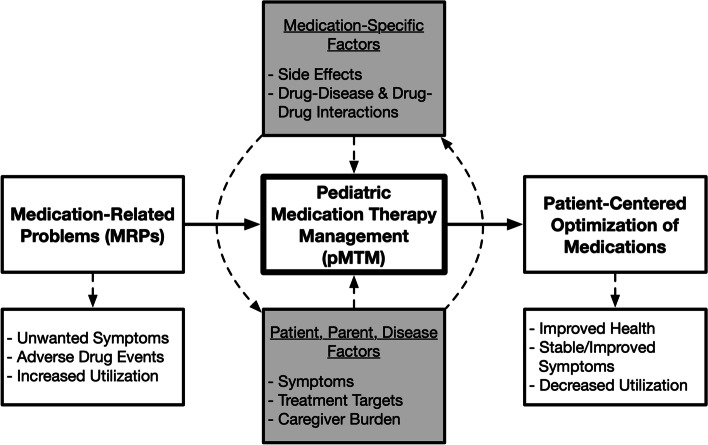
Background: Children with medical complexity (CMC) often rely upon the use of multiple medications to sustain quality of life and control substantial symptom burden. Pediatric polypharmacy (≥ 5 concurrent medications) is prevalent and increases the risk of medication-related problems (MRPs). Although MRPs are associated with pediatric morbidity and healthcare utilization, polypharmacy is infrequently assessed during routine clinical care for CMC. The aim of this randomized controlled trial is to determine if a structured pharmacist-led Pediatric Medication Therapy Management (pMTM) intervention reduces MRP counts, as well as the secondary outcomes of symptom burden and acute healthcare utilization.
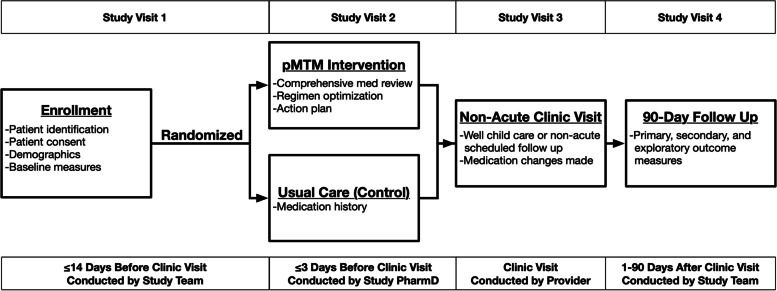
Methods: This is a hybrid type 2 randomized controlled trial assessing the effectiveness of pMTM compared to usual care in a large, patient-centered medical home for CMC. Eligible patients include all children ages 2-18 years old, with ≥ 1 complex chronic condition, and with ≥ 5 active medications, as well as their English-speaking primary caregivers. Child participants and their primary parental caregivers will be randomized to pMTM or usual care before a non-acute primary care visit and followed for 90 days. Using generalized linear models, the overall effectiveness of the intervention will be evaluated using total MRP counts at 90 days following pMTM intervention or usual care visit. Following attrition, a total of 296 CMC will contribute measurements at 90 days, which provides > 90% power to detect a clinically significant 1.0 reduction in total MRPs with an alpha level of 0.05. Secondary outcomes include Parent-Reported Outcomes of Symptoms (PRO-Sx) symptom burden scores and acute healthcare visit counts. Program replication costs will be assessed using time-driven activity-based scoring.
Discussion: This pMTM trial aims to test hypotheses that a patient-centered medication optimization intervention delivered by pediatric pharmacists will result in lower MRP counts, stable or improved symptom burdens, and fewer cumulative acute healthcare encounters at 90 days following pMTM compared to usual care. The results of this trial will be used to quantify medication-related outcomes, safety, and value for a high-utilization group of CMC, and outcomes may elucidate the role of integrated pharmacist services as a key component of outpatient complex care programs for this priority pediatric population.
Trial registration: This trial was prospectively registered at clinicaltrials.gov (NCT05761847) on Feb 25, 2023.
Keywords: Adverse drug events; Children with medical complexity; Deprescribing; Medication safety; Pediatrics; Polypharmacy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Feinstein JA, Hall M, Antoon JW, Thomson J, Flores JC, Goodman DM, Cohen E, Azuine R, Agrawal R, Houtrow AJ, DeCourcey DD, Kuo DZ, Coller R, Gaur DS, Berry JG. Chronic Medication Use in Children Insured by Medicaid: A Multistate Retrospective Cohort Study. Pediatrics. 2019;143(4). 10.1542/peds.2018-3397. Epub 2019/03/28. PubMed PMID: 30914443; PMCID: PMC6456893. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
