

Burden of lipoprotein(a) for patients with atherosclerotic cardiovascular disease: A retrospective analysis from the United States
- PMID: 37121256
- PMCID: PMC10387958
- DOI: 10.18553/jmcp.2023.29.5.519
Burden of lipoprotein(a) for patients with atherosclerotic cardiovascular disease: A retrospective analysis from the United States
Abstract
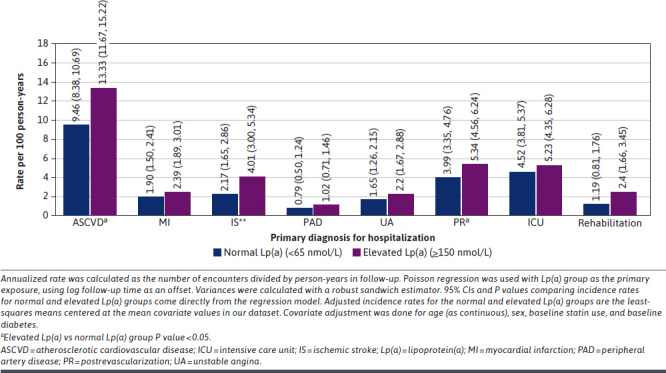
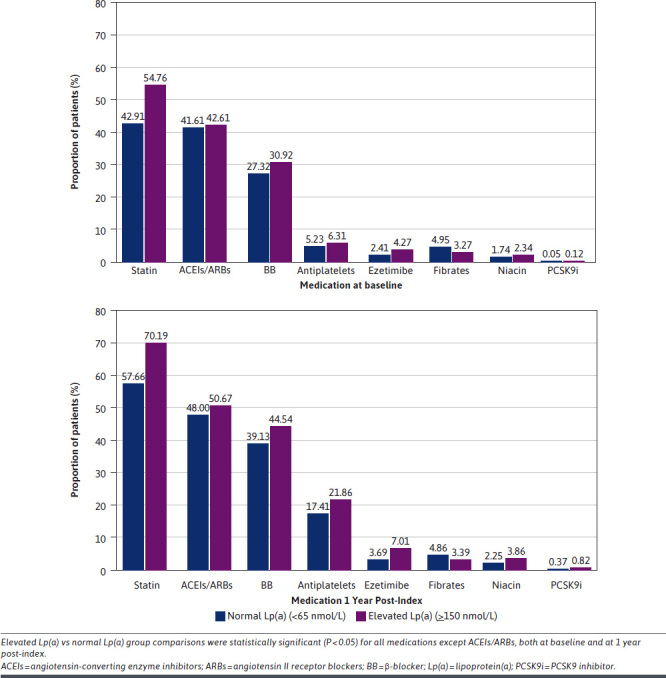
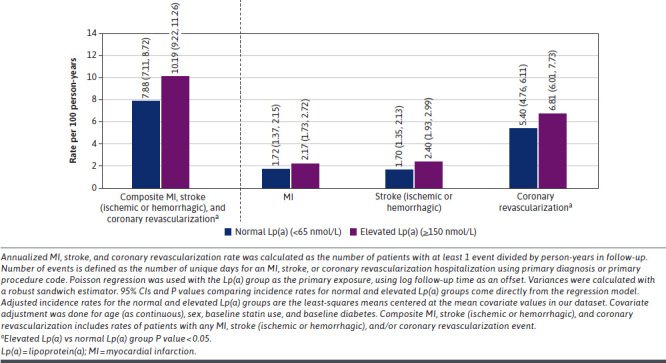
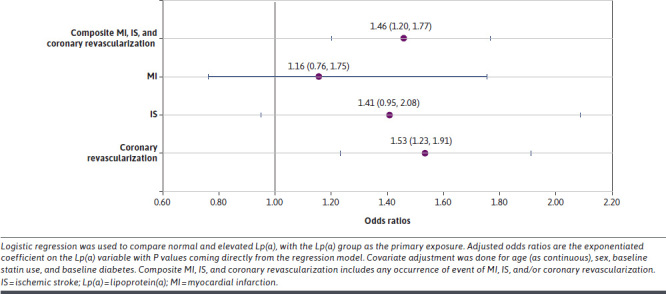
BACKGROUND: Lipoprotein(a) (Lp(a)) is an inherited, independent, and causal risk factor for atherosclerotic cardiovascular disease (ASCVD). OBJECTIVE: To assess the burden of elevated Lp(a) for patients with ASCVD in a real-world setting in the United States. METHODS: This retrospective cohort study assessed US patients with available Lp(a) measurement and established ASCVD using Optum's Clinformatics Data Mart database (2007-2020). Index date was defined as the first diagnosis of an ASCVD event. Patient demographics, medications, health care resource utilization (HCRU), and occurrence of cardiovascular events were assessed for patients with elevated (≥150 nmol/L) vs normal (≥65 nmol/L) Lp(a) levels, within the first year of index date. HCRU was characterized by inpatient hospitalization, inpatient length of stay (LOS), outpatient visits, and emergency department (ED) visits. All comparative analyses of patients with elevated (≥150 nmol/L) vs normal (≥65 nmol/L) Lp(a) levels within the first year of index date were adjusted for age, sex, baseline statin use, and diabetes. RESULTS: 8,372 patients with ASCVD and Lp(a) measurement in nmol/L were included in this study. Patient demographics and baseline clinical characteristics were similar among those with normal and elevated Lp(a). However, the proportion of patients receiving statins and β-blockers at baseline were significantly higher in the elevated vs normal Lp(a) group (54.76% vs 42.91%, P < 0.0001, and 30.92% vs 27.32%, P = 0.0183, respectively). At 1 year of follow-up, the rates per 100 person-years for ASCVD-related inpatient hospitalizations, outpatient hospitalizations, and ED visits were higher among patients with elevated Lp(a) compared with normal Lp(a) (13.33 vs 9.46, 89.08 vs 85.10, and 2.89 vs 2.29, respectively). The mean LOS per ASCVD-related hospitalization was 7.21 days in the elevated and 6.26 days in the normal Lp(a) group (P = 0.3462). During the 1-year post-index follow-up period, 15% of patients in the elevated Lp(a) group required revascularization compared with 10% of patients in the normal Lp(a) group (P = 0.0002). The odds of composite myocardial infarction, ischemic stroke, and revascularization occurrence of events within the first year of index was significantly higher in the elevated Lp(a) group compared with the normal Lp(a) group (1.46; 95% CI = 1.20-1.77; P < 0.05). CONCLUSIONS: HCRU within the first year of ASCVD diagnosis is substantial among patients with ASCVD and elevated Lp(a). Relatively higher rates of inpatient hospitalizations, increased LOS per hospitalization, and requirement of revascularization procedures within the first year of ASCVD index diagnosis were observed in patients with elevated Lp(a) compared with normal Lp(a) levels. Lp(a) testing in routine clinical practice could help in identification of high-risk patients with ASCVD and play an important role in the overall cardiovascular risk management, aiming to reduce the HCRU associated with ASCVD. DISCLOSURES: Ms Fonseca, Dr Laguna, Dr Itani, Dr Rachel Studer, and Dr Ferber are employees of Novartis Pharma AG, Basel, Switzerland. Ms Byrne is an employee of Novartis AG, Dublin, Ireland. Dr Costa-Scharplatz is an employee of Novartis Sweden AB, Stockholm, Sweden. Dr Heo and Ms Dillon are employees of Genesis Research. Genesis Research was commissioned to conduct the study (data extraction and analysis) on behalf of Novartis Pharma AG.
Conflict of interest statement
Ms Fonseca, Dr Laguna, Dr Itani, Dr Rachel Studer, and Dr Ferber are employees of Novartis Pharma AG, Basel, Switzerland. Ms Byrne is an employee of Novartis AG, Dublin, Ireland. Dr Costa-Scharplatz is an employee of Novartis Sweden AB, Stockholm, Sweden. Dr Heo and Ms Dillon are employees of Genesis Research. Genesis Research was commissioned to conduct the study (data extraction and analysis) on behalf of Novartis Pharma AG.
Figures
References
-
- Tsimikas S. A test in context: Lipoprotein(a): Diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol. 2017;69(6):692-711. doi:10.1016/j.jacc.2016.11.042 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
