

Molecular markers of metastatic disease in KRAS-mutant lung adenocarcinoma
- PMID: 37121400
- PMCID: PMC10425882
- DOI: 10.1016/j.annonc.2023.04.514
Molecular markers of metastatic disease in KRAS-mutant lung adenocarcinoma
Abstract
Background: Prior studies characterized the association of molecular alterations with treatment-specific outcomes in KRAS-mutant (KRASMUT) lung adenocarcinoma (LUAD). Less is known about the prognostic role of molecular alterations and their associations with metastatic disease.
Patients and methods: We analyzed clinicogenomic data from 1817 patients with KRASMUT LUAD sequenced at the Dana-Farber Cancer Institute (DFCI) and Memorial Sloan Kettering Cancer Center (MSKCC). Patients with metastatic (M1) and nonmetastatic (M0) disease were compared. Transcriptomic data from The Cancer Genome Atlas (TCGA) were investigated to characterize the biology of differential associations with clinical outcomes. Organ-specific metastasis was associated with overall survival (OS).
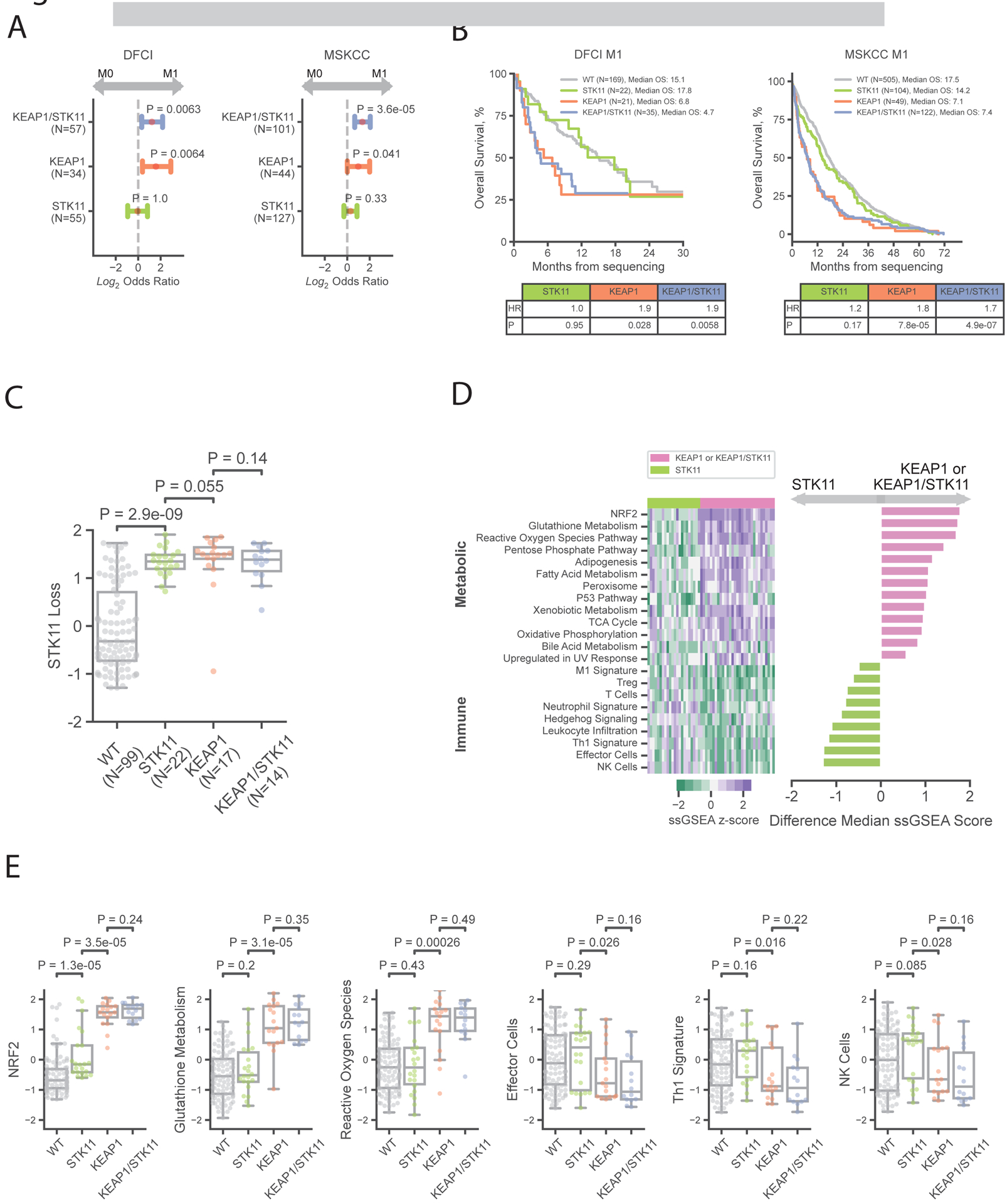
Results: KEAP1 (DFCI: OR = 2.3, q = 0.04; MSKCC: OR = 2.2, q = 0.00027) and SMARCA4 mutations (DFCI: OR = 2.5, q = 0.06; MSKCC: OR = 2.6, q = 0.0021) were enriched in M1 versus M0 tumors. On integrative modeling, NRF2 activation was the genomic feature most associated with OS. KEAP1 mutations were enriched in M1 versus M0 tumors independent of STK11 status (KEAP1MUT/STK11WT: DFCI OR = 3.0, P = 0.0064; MSKCC OR = 2.0, P = 0.041; KEAP1MUT/STK11MUT: DFCI OR = 2.3, P = 0.0063; MSKCC OR = 2.5, P = 3.6 × 10-05); STK11 mutations without KEAP1 loss were not associated with stage (KEAP1WT/STK11MUT: DFCI OR = 0.97, P = 1.0; MSKCC OR = 1.2, P = 0.33) or outcome. KEAP1/KRAS-mutated tumors with and without STK11 mutations exhibited high functional STK11 loss. The negative effects of KEAP1 were compounded in the presence of bone (HR = 2.3, P = 4.4 × 10-14) and negated in the presence of lymph node metastasis (HR = 1.0, P = 0.91).
Conclusions: Mutations in KEAP1 and SMARCA4, but not STK11, were associated with metastatic disease and poor OS. Functional STK11 loss, however, may contribute to poor outcomes in KEAP1MUT tumors. Integrating molecular data with clinical and metastatic-site annotations can more accurately risk stratify patients.
Keywords: KEAP1; KRAS; STK11; lung adenocarcinoma; metastatic.
Copyright © 2023 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures




References
-
- Skoulidis F, Byers LA, Diao L, Papadimitrakopoulou VA, Tong P, Izzo J, et al. Co-occurring Genomic Alterations Define Major Subsets of KRAS-Mutant Lung Adenocarcinoma with Distinct Biology, Immune Profiles, and Therapeutic Vulnerabilities [Internet]. Vol. 5, Cancer Discovery. 2015; 860–877. Available at: 10.1158/2159-8290.cd-14-1236 - DOI - PMC - PubMed
-
- Skoulidis F, Li BT, Dy GK, Price TJ, Falchook GS, Wolf J, et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation. N Engl J Med. June 4, 2021. [cited June 24, 2022]; Available at: https://www.nejm.org/doi/full/10.1056/NEJMoa2103695 - DOI - PMC - PubMed
-
- Arbour KC, Jordan E, Kim HR, Dienstag J, Yu HA, Sanchez-Vega F, et al. Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non–Small Cell Lung Cancer [Internet]. Vol. 24, Clinical Cancer Research. 2018; 334–340. Available at: 10.1158/1078-0432.ccr-17-1841 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
