

Optimizing spine surgery instrument trays to immediately increase efficiency and reduce costs in the operating room
- PMID: 37124067
- PMCID: PMC10130344
- DOI: 10.1016/j.xnsj.2023.100208
Optimizing spine surgery instrument trays to immediately increase efficiency and reduce costs in the operating room
Abstract
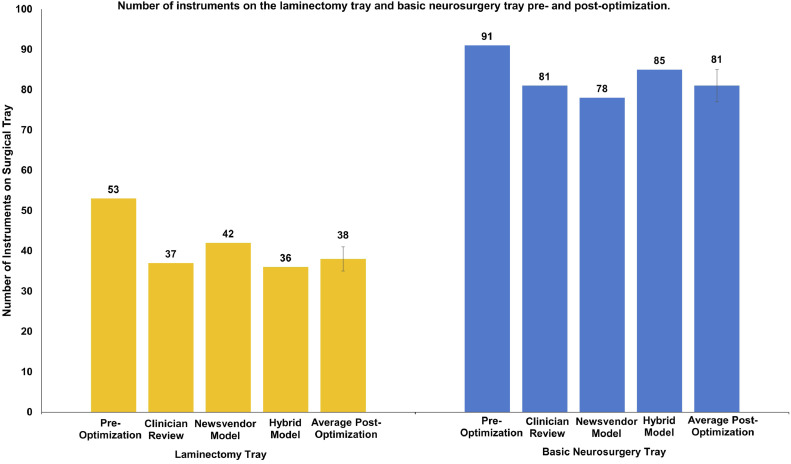
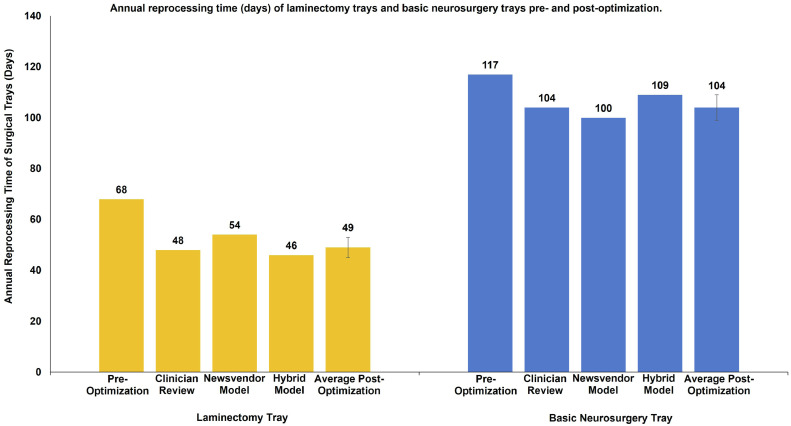
Background: Over-crowded surgical trays result in perioperative inefficiency and unnecessary costs. While methodologies to reduce the size of surgical trays have been described in the literature, they each have their own drawbacks. In this study, we compared three methods: (1) clinician review (CR), (2) mathematical programming (MP), and (3) a novel hybrid model (HM) based on surveys and cost analysis. While CR and MP are well documented, CR can yield suboptimal reductions and MP can be laborious and technically challenging. We hypothesized our easy-to-implement HM would result in a reduction of surgical instruments in both the laminectomy tray (LT) and basic neurosurgery tray (BNT) that is comparable to CR and MP.
Methods: Three approaches were tested: CR, MP, and HM. We interviewed 5 neurosurgeons and 3 orthopedic surgeons, at our institution, who performed a total of 5437 spine cases, requiring the use of the LT and BNT over a 4-year (2017-2021) period. In CR, surgeons suggested which surgical instruments should be removed. MP was performed via the mathematical analysis of 25 observations of the use of a LT and BNT tray. The HM was performed via a structured survey of the surgeons' estimated instrument usage, followed by a cost-based inflection point analysis.
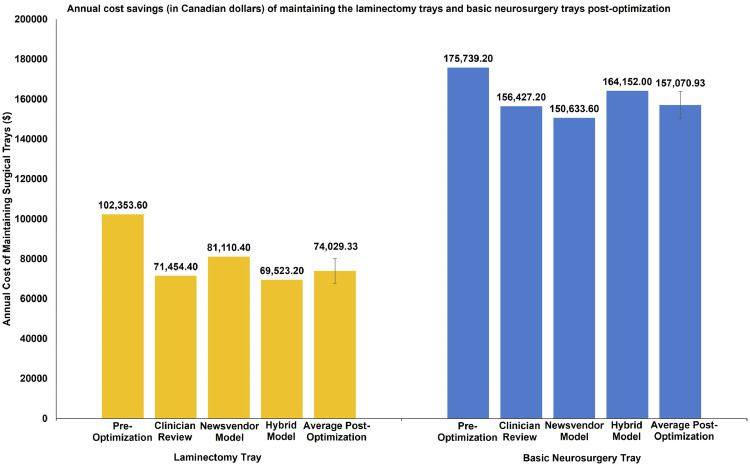
Results: The CR, MP, and HM approaches resulted in a total instrument reduction of 41%, 35%, and 38%, respectively, corresponding to total cost savings per annum of $50,211.20, $46,348.80, and $44,417.60, respectively.
Conclusions: While hospitals continue to examine perioperative services for potential inefficiencies, surgical inventory will be increasingly scrutinized. Despite MP being the most accurate methodology to do so, our results suggest that savings were similar across all three methods. CR and HM are significantly less laborious and thus are practical alternatives.
Keywords: Clinician review; Cost savings; Mathematical model; Newsvendor model; Optimization; Spine surgery; Standardization; Surgical instruments; Surgical trays.
© 2023 Published by Elsevier Ltd on behalf of North American Spine Society.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Daultani Y., Chaudhuri A., Kumar S. A decade of lean in healthcare: current state and future directions. Glob Bus Rev. 2015;16:1082–1099. doi: 10.1177/0972150915604520. - DOI
-
- Timmermans S., Epstein S. A world of standards but not a standard world: toward a sociology of standards and standardization. Annu Rev Sociol. 2010;36:69–89. doi: 10.1146/ANNUREV.SOC.012809.102629. - DOI
-
- De Regge M., Gemmel P., Meijboom B. How operations matters in healthcare standardization. Int J Oper Prod Manag. 2019;39:1144–1165. doi: 10.1108/IJOPM-03-2019-0227. - DOI
LinkOut - more resources
Full Text Sources
