

Association of late gadolinium enhancement in cardiac magnetic resonance with mortality, ventricular arrhythmias, and heart failure in patients with nonischemic cardiomyopathy: A systematic review and meta-analysis
- PMID: 37124560
- PMCID: PMC10134398
- DOI: 10.1016/j.hroo.2023.01.001
Association of late gadolinium enhancement in cardiac magnetic resonance with mortality, ventricular arrhythmias, and heart failure in patients with nonischemic cardiomyopathy: A systematic review and meta-analysis
Abstract
Background: Late gadolinium enhancement (LGE) on cardiac magnetic resonance is a predictor of adverse events in patients with nonischemic cardiomyopathy (NICM).
Objective: This meta-analysis evaluated the correlation between LGE and mortality, ventricular arrhythmias (VAs) and sudden cardiac death (SCD), and heart failure (HF) outcomes.
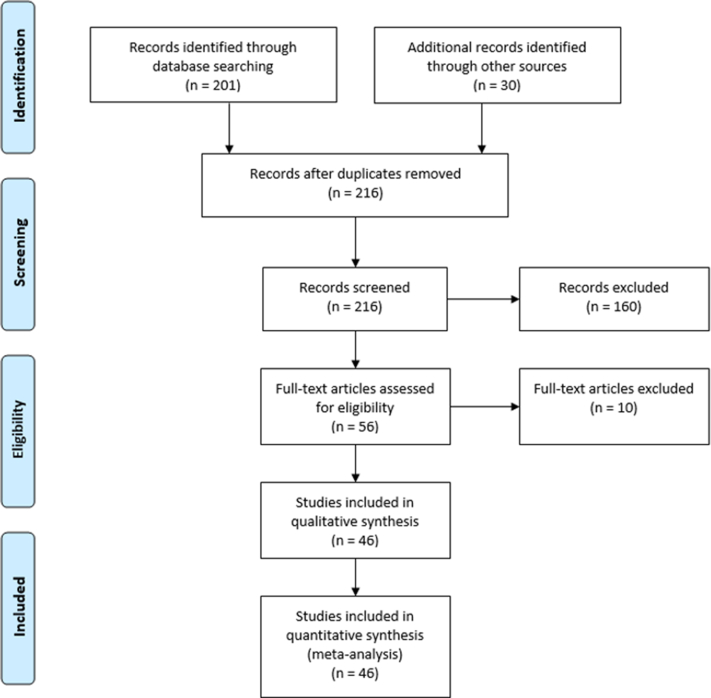
Methods: A literature search was conducted for studies reporting the association between LGE in NICM and the study endpoints. The primary endpoint was mortality. Secondary endpoints included VA and SCD, HF hospitalization, improvement in left ventricular ejection fraction (LVEF) to >35%, and heart transplantation referral. The search was not restricted to time or publication status. The minimum follow-up duration was 1 year.
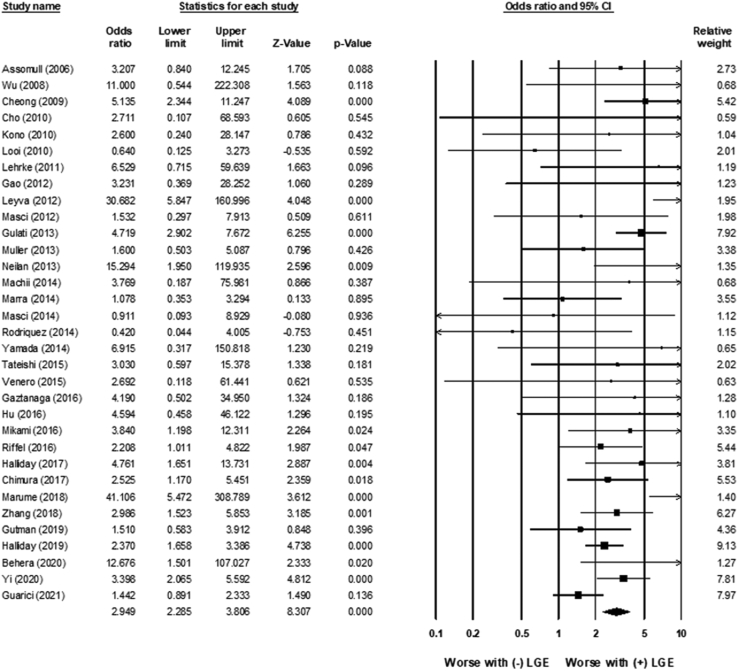
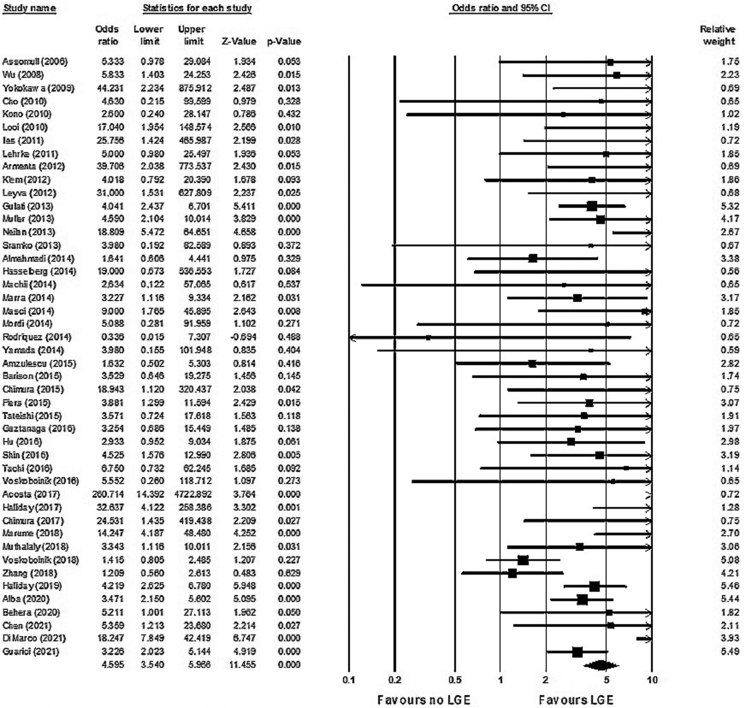
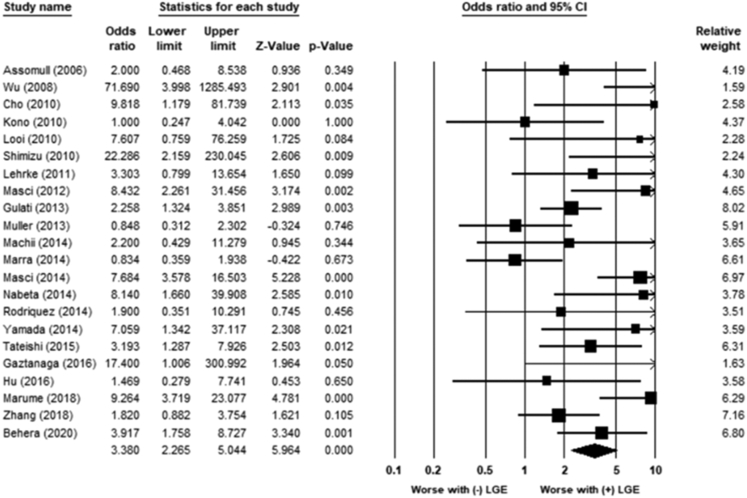
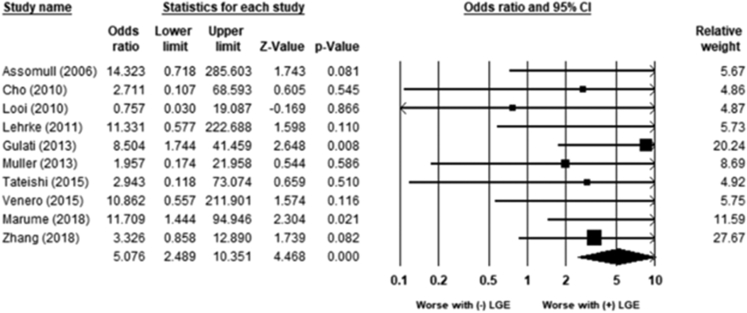
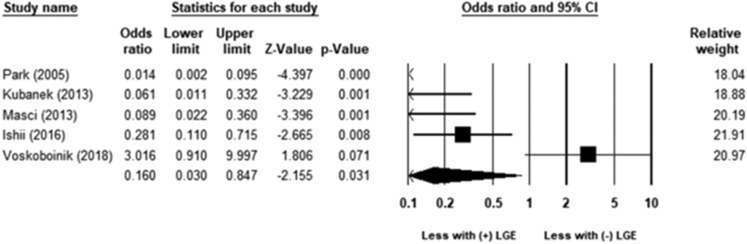
Results: A total of 46 studies and 10,548 NICM patients (4610 with LGE, 5938 without LGE) were included; mean follow-up was 3 years (range 13-71 months). LGE was associated with increased mortality (odds ratio [OR] 2.9; 95% confidence interval [CI] 2.3-3.8; P < .01) and VA and SCD (OR 4.6; 95% CI 3.5-6.0; P < .01). LGE was associated with an increased risk of HF hospitalization (OR 3.4; 95% CI 2.3-5.0; P < .01), referral for transplantation (OR 5.1; 95% CI 2.5-10.4; P < .01), and decreased incidence of LVEF improvement to >35% (OR 0.2; 95% CI 0.03-0.85; P = .03).
Conclusion: LGE in NICM patients is associated with increased mortality, VA and SCD, and HF hospitalization and heart transplantation referral during long-term follow up. Given these competing risks of mortality and HF progression, prospective randomized controlled trials are required to determine if LGE is useful for guiding prophylactic implantable cardioverter-defibrillator placement in NICM patients.
Keywords: CMR; LGE; Mortality; Ventricular arrhythmia.
© 2023 Heart Rhythm Society. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
