

Surgical outcomes of gallbladder cancer: the OMEGA retrospective, multicentre, international cohort study
- PMID: 37125405
- PMCID: PMC10130604
- DOI: 10.1016/j.eclinm.2023.101951
Surgical outcomes of gallbladder cancer: the OMEGA retrospective, multicentre, international cohort study
Abstract
Background: Gallbladder cancer (GBC) is rare but aggressive. The extent of surgical intervention for different GBC stages is non-uniform, ranging from cholecystectomy alone to extended resections including major hepatectomy, resection of adjacent organs and routine extrahepatic bile duct resection (EBDR). Robust evidence here is lacking, however, and survival benefit poorly defined. This study assesses factors associated with recurrence-free survival (RFS), overall survival (OS) and morbidity and mortality following GBC surgery in high income countries (HIC) and low and middle income countries (LMIC).
Methods: The multicentre, retrospective Operative Management of Gallbladder Cancer (OMEGA) cohort study included all patients who underwent GBC resection across 133 centres between 1st January 2010 and 31st December 2020. Regression analyses assessed factors associated with OS, RFS and morbidity.
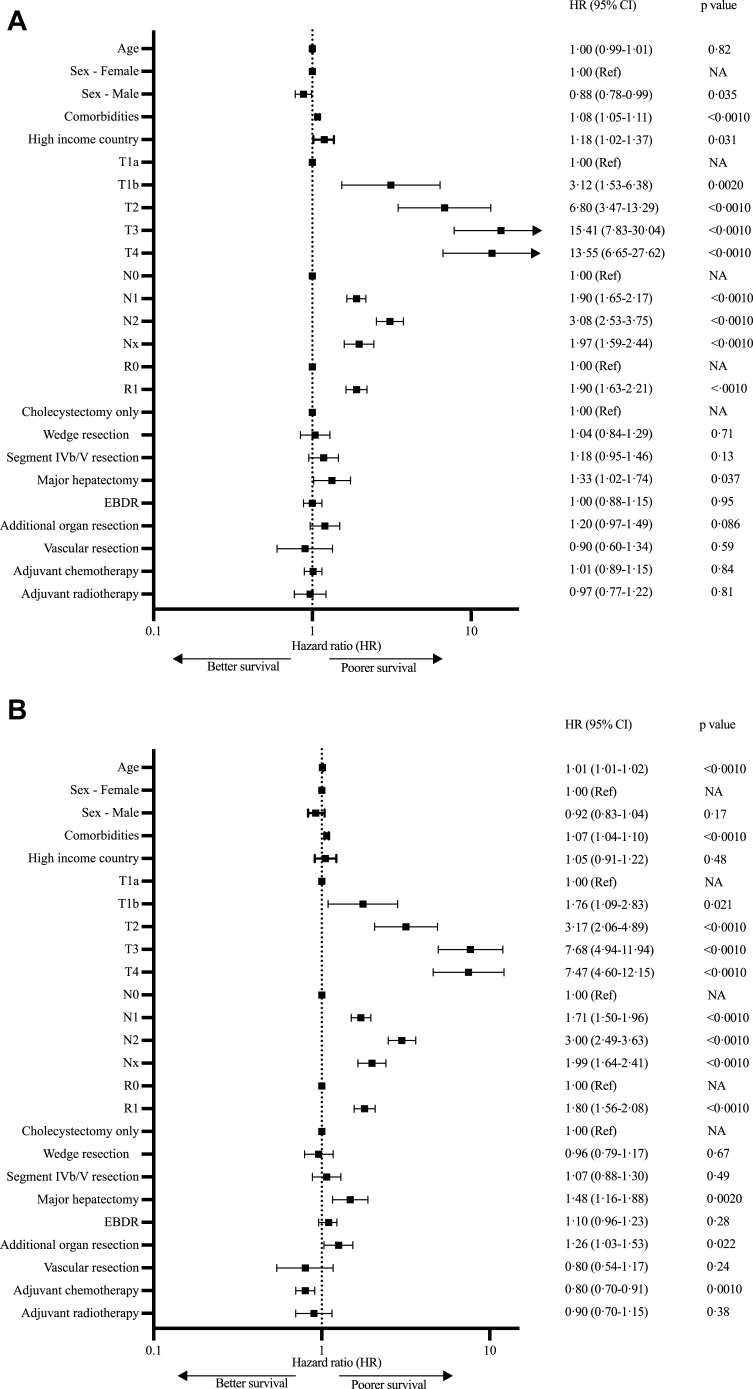
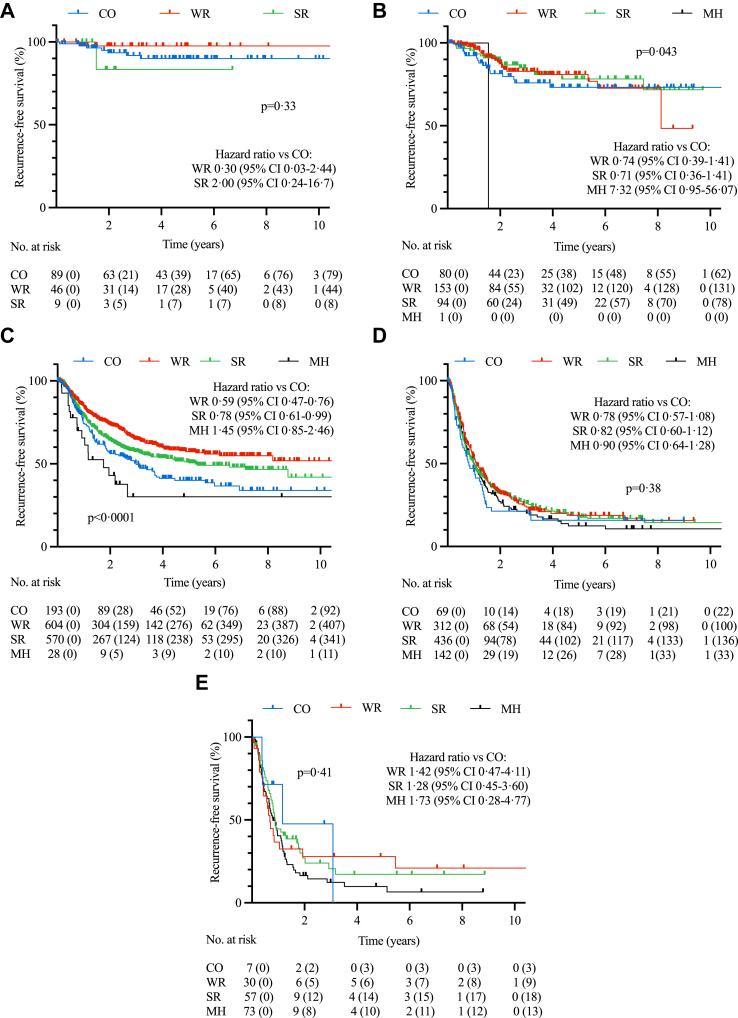
Findings: On multivariable analysis of all 3676 patients, wedge resection and segment IVb/V resection failed to improve RFS (HR 1.04 [0.84-1.29], p = 0.711 and HR 1.18 [0.95-1.46], p = 0.13 respectively) or OS (HR 0.96 [0.79-1.17], p = 0.67 and HR 1.48 [1.16-1.88], p = 0.49 respectively), while major hepatectomy was associated with worse RFS (HR 1.33 [1.02-1.74], p = 0.037) and OS (HR 1.26 [1.03-1.53], p = 0.022). Furthermore, EBDR (OR 2.86 [2.3-3.52], p < 0.0010), resection of additional organs (OR 2.22 [1.62-3.02], p < 0.0010) and major hepatectomy (OR 3.81 [2.55-5.73], p < 0.0010) were all associated with increased morbidity and mortality. Compared to LMIC, patients in HIC were associated with poorer RFS (HR 1.18 [1.02-1.37], p = 0.031) but not OS (HR 1.05 [0.91-1.22], p = 0.48). Adjuvant and neoadjuvant treatments were infrequently used.
Interpretation: In this large, multicentre analysis of GBC surgical outcomes, liver resection was not conclusively associated with improved survival, and extended resections were associated with greater morbidity and mortality without oncological benefit. Aggressive upfront resections do not benefit higher stage GBC, and international collaborations are needed to develop evidence-based neoadjuvant and adjuvant treatment strategies to minimise surgical morbidity and prioritise prognostic benefit.
Funding: Cambridge Hepatopancreatobiliary Department Research Fund.
Keywords: Cholangiocarcinoma; Gallbladder cancer; Liver resection; Surgical outcomes.
© 2023 The Author(s).
Conflict of interest statement
SM has the following interests: 1) Principal investigator of a clinical trial on intrahepatic cholangiocarcinoma funded by BMS/Celgene (grant funding provided to institution, no personal compensation) 2) Advisory board member at Astra Zeneca on management of hepatocellular carcinoma and 3) Scientific Medical Advisory Board member Cholangiocarcinoma Foundation. None of the authors have any conflicts of interests to declare.
Figures


References
-
- Ferlay J., Ervik M., Lam F., et al. International Agency for Research on Cancer; Lyon, France: 2020. Global cancer observatory: cancer today.https://gco.iarc.fr/today
-
- Alrawashdeh W., Kamarajah S.K., Gujjuri R.R., et al. Systematic review and meta-analysis of survival outcomes in T2a and T2b gallbladder cancers. HPB (Oxford) 2022;24:789–796. - PubMed
-
- Lee H., Kwon W., Han Y., Kim J.R., Kim S.-W., Jang J.-Y. Optimal extent of surgery for early gallbladder cancer with regard to long-term survival: a meta-analysis. J Hepatobiliary Pancreat Sci. 2018;25:131–141. - PubMed
-
- Meara J.G., Leather A.J.M., Hagander L., et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386:569–624. - PubMed
LinkOut - more resources
Full Text Sources
