

Identification of a Common Variant for Coronary Heart Disease at PDE1A Contributes to Individualized Treatment Goals and Risk Stratification of Cardiovascular Complications in Chinese Patients With Type 2 Diabetes
- PMID: 37125963
- PMCID: PMC10234754
- DOI: 10.2337/dc22-2331
Identification of a Common Variant for Coronary Heart Disease at PDE1A Contributes to Individualized Treatment Goals and Risk Stratification of Cardiovascular Complications in Chinese Patients With Type 2 Diabetes
Abstract
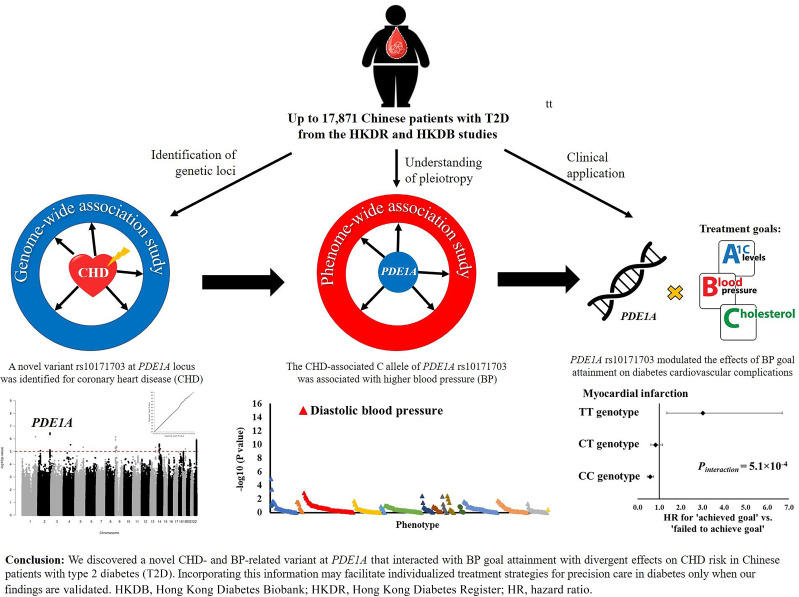
Objective: In this study we aim to unravel genetic determinants of coronary heart disease (CHD) in type 2 diabetes (T2D) and explore their applications.
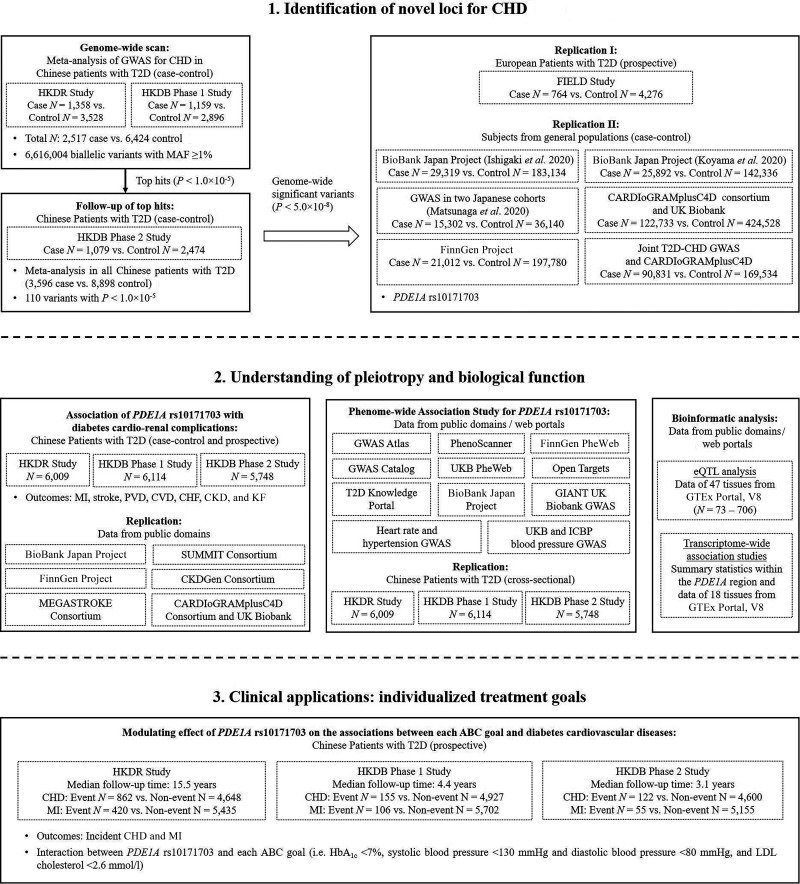
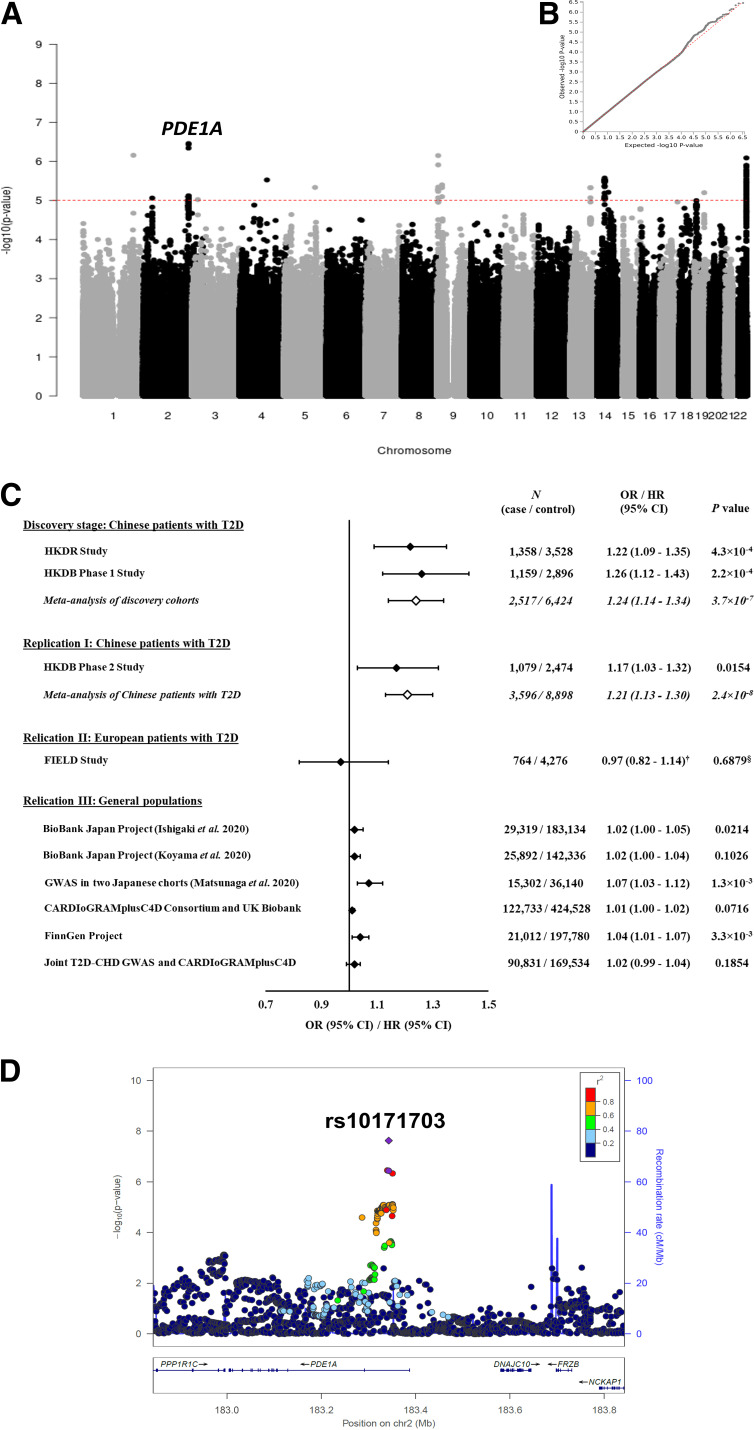
Research design and methods: We performed a two-stage genome-wide association study for CHD in Chinese patients with T2D (3,596 case and 8,898 control subjects), followed by replications in European patients with T2D (764 case and 4,276 control subjects) and general populations (n = 51,442-547,261). Each identified variant was examined for its association with a wide range of phenotypes and its interactions with glycemic, blood pressure (BP), and lipid controls in incident cardiovascular diseases.
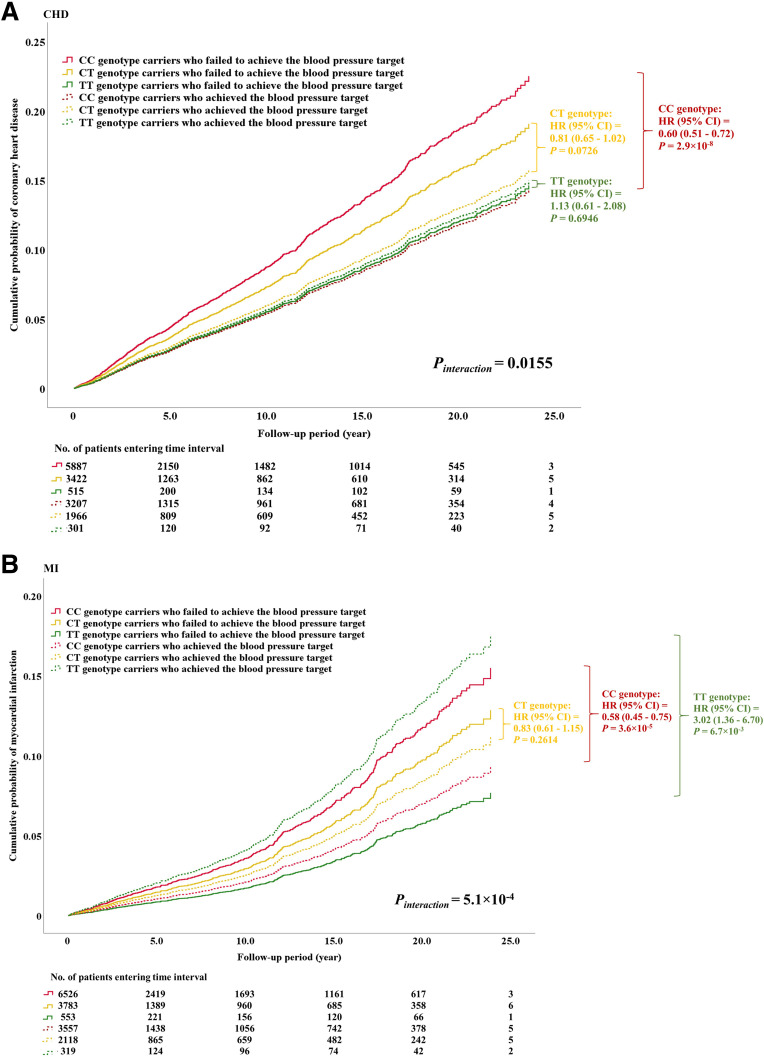
Results: We identified a novel variant (rs10171703) for CHD (odds ratio 1.21 [95% CI 1.13-1.30]; P = 2.4 × 10-8) and BP (β ± SE 0.130 ± 0.017; P = 4.1 × 10-14) at PDE1A in Chinese T2D patients but found only a modest association with CHD in general populations. This variant modulated the effects of BP goal attainment (130/80 mmHg) on CHD (Pinteraction = 0.0155) and myocardial infarction (MI) (Pinteraction = 5.1 × 10-4). Patients with CC genotype of rs10171703 had >40% reduction in either cardiovascular events in response to BP control (2.9 × 10-8 < P < 3.6 × 10-5), those with CT genotype had no difference (0.0726 < P < 0.2614), and those with TT genotype had a threefold increase in MI risk (P = 6.7 × 10-3).
Conclusions: We discovered a novel CHD- and BP-related variant at PDE1A that interacted with BP goal attainment with divergent effects on CHD risk in Chinese patients with T2D. Incorporating this information may facilitate individualized treatment strategies for precision care in diabetes, only when our findings are validated.
© 2023 by the American Diabetes Association.
Conflict of interest statement
Figures
References
-
- Peters SAE, Huxley RR, Woodward M. Diabetes as risk factor for incident coronary heart disease in women compared with men: a systematic review and meta-analysis of 64 cohorts including 858,507 individuals and 28,203 coronary events. Diabetologia 2014;57:1542–1551 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
