

Telesurgery and telesurgical support using a double-surgeon cockpit system allowing manipulation from two locations
- PMID: 37126192
- PMCID: PMC10150667
- DOI: 10.1007/s00464-023-10061-6
Telesurgery and telesurgical support using a double-surgeon cockpit system allowing manipulation from two locations
Abstract
Background: Although several studies on telesurgery have been reported globally, a clinically applicable technique has not yet been developed. As part of a telesurgical study series conducted by the Japan Surgical Society, this study describes the first application of a double-surgeon cockpit system to telesurgery.
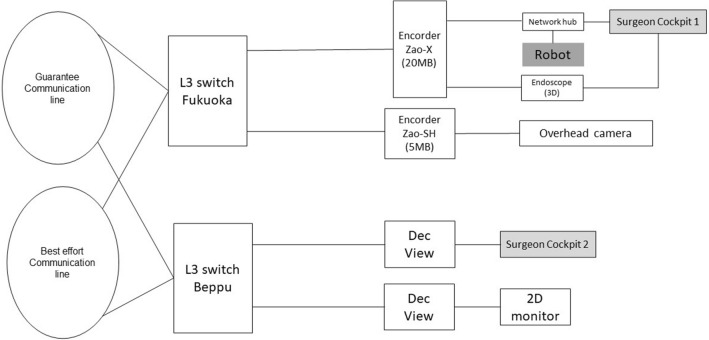
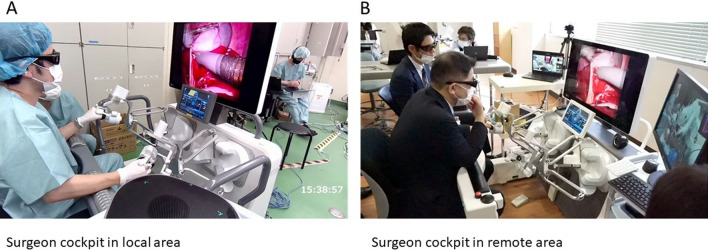
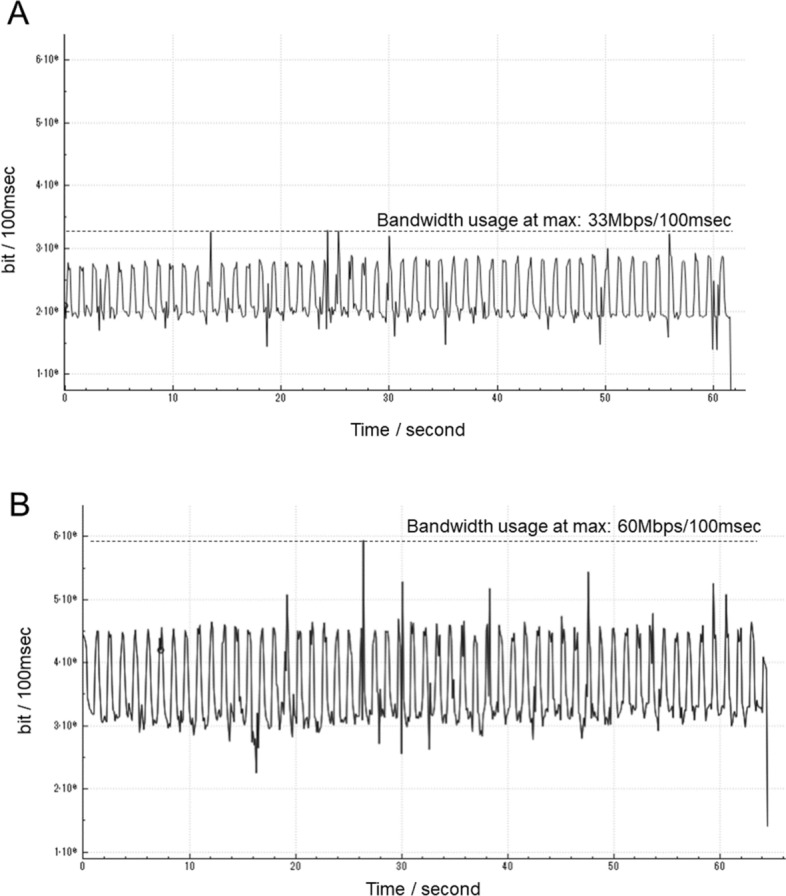
Methods: Surgeon cockpits were installed at a local site and a remote site 140 km away. Three healthy pigs weighing between 26 and 29 kg were selected for surgery. Non-specialized surgeons performed emergency hemostasis, cholecystectomy, and renal vein ligation with remote assistance using the double-surgeon cockpits and specialized surgeons performed actual telesurgery. Additionally, the impact of adding internet protocol security (IPsec) encryption to the internet protocol-virtual private network (IP-VPN) line on communication was evaluated to address clinical security concerns.
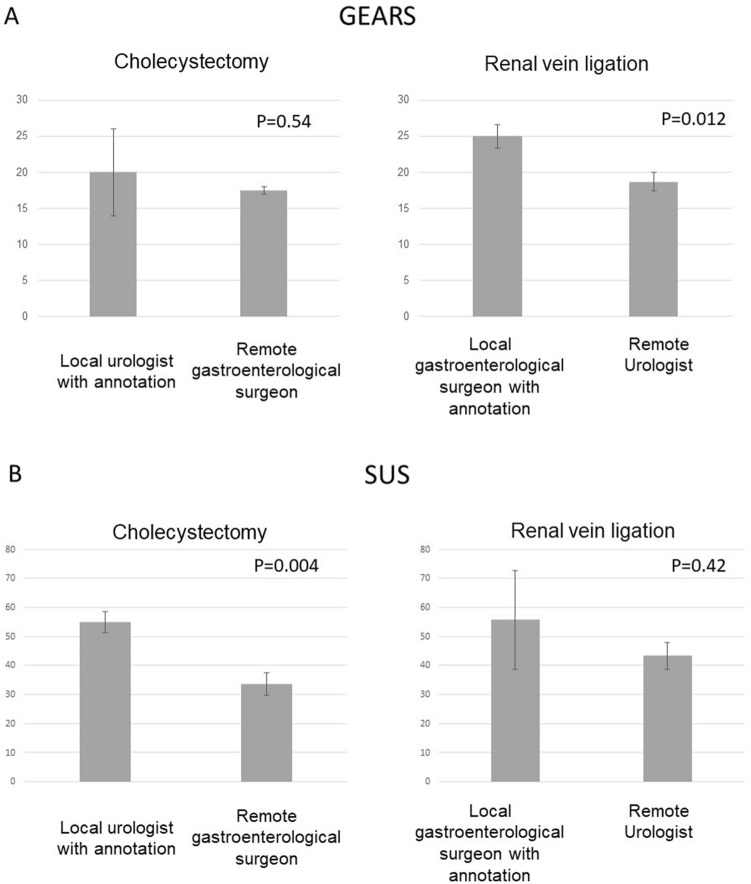
Results: The average time required for remote emergency hemostasis with the double-surgeon cockpit system was 10.64 s. A non-specialized surgeon could safely perform cholecystectomy or renal vein ligation with remote assistance. Global Evaluative Assessment of Robotic Skills and System Usability Scale scores were higher for telesurgical support-assisted surgery by a non-specialized surgeon using the double-surgeon cockpits than for telesurgery performed by a specialized surgeon without the double-cockpit system. Adding IPsec encryption to the IP-VPN did not have a significant impact on communication.
Conclusion: Telesurgical support through our double-surgeon cockpit system is feasible as first step toward clinical telesurgery.
Keywords: Double-surgeon cockpit; Telementoring; Telesurgery; Telesurgical support.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Drs. Eiji Oki, Mitsuhiko Ota, Tomonori Nakanoko, Yasushi Tanaka, Satoshi Toyota, Qingjiang Hu, Yu Nakaji, Ryota Nakanishi, Koji Ando, Yasue Kimura, Yuichi Hisamatsu, Koshi Mimori, Yoshiya Takahashi, Hajime Morohashi, Kotaro Tadano, Hironobu Takano, Yuma Ebihara, Masaki Shiota, Junichi Inokuchi, Masatoshi Eto, Tomoharu Yoshizumi, Satoshi Hirano, and Masaki Mori have no conflicts of interest or financial ties to disclose. Takahiro Kanno and Kenji Kawashima received stock options from Riverfield, Inc. Kenichi Hakamada has received research funding from AMED and honoraria for lectures and manuscripts from the following organizations: Japan Medical Association, Keidanren, NTT East Corporation, Nankodo, Tokyo Igakusha, and Medical Sciences International.
Figures
References
-
- Kirkpatrick AW, McKee JL, Tomlinson C, Donley N, Ball CG, Wachs J. A randomized controlled pilot trial of video-modelling versus telementoring for improved hemorrhage control wound packing. Am J Surg. 2022;5:00097–96. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
