

Effects of a Multimodal Transitional Care Intervention in Patients at High Risk of Readmission: The TARGET-READ Randomized Clinical Trial
- PMID: 37126338
- PMCID: PMC10152373
- DOI: 10.1001/jamainternmed.2023.0791
Effects of a Multimodal Transitional Care Intervention in Patients at High Risk of Readmission: The TARGET-READ Randomized Clinical Trial
Abstract
Importance: Hospital readmissions are frequent, costly, and sometimes preventable. Although these issues have been well publicized and incentives to reduce them introduced, the best interventions for reducing readmissions remain unclear.
Objectives: To evaluate the effects of a multimodal transitional care intervention targeting patients at high risk of hospital readmission on the composite outcome of 30-day unplanned readmission or death.
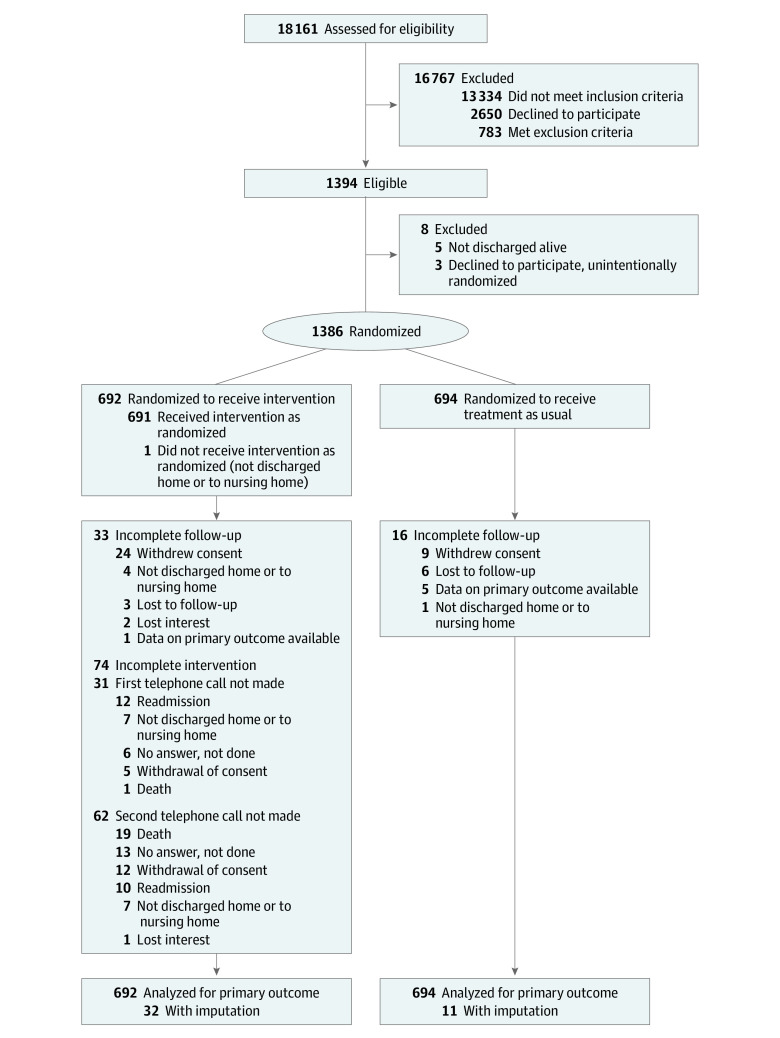
Design, setting, and participants: A single-blinded, multicenter randomized clinical trial was conducted from April 2018 to January 2020, with a 30-day follow-up in 4 medium-to-large-sized teaching hospitals in Switzerland. Participants were consecutive patients discharged from general internal medicine wards and at higher risk of unplanned readmission based on their simplified HOSPITAL score (≥4 points). Data were analyzed between April and September 2022.
Interventions: The intervention group underwent systematic medication reconciliation, a 15-minute patient education session with teach-back, a planned first follow-up visit with their primary care physician, and postdischarge follow-up telephone calls from the study team at 3 and 14 days. The control group received usual care from their hospitalist, plus a 1-page standard study information sheet.
Main outcomes and measures: Thirty-day postdischarge unplanned readmission or death.
Results: A total of 1386 patients were included with a mean (SD) age of 72 (14) years; 712 (51%) were male. The composite outcome of 30-day unplanned readmission or death was 21% (95% CI, 18% to 24%) in the intervention group and 19% (95% CI, 17% to 22%) in the control group. The intention-to-treat analysis risk difference was 1.7% (95% CI, -2.5% to 5.9%; P = .44). There was no evidence of any intervention effects on time to unplanned readmission or death, postdischarge health care use, patient satisfaction with the quality of their care transition, or readmission costs.
Conclusions and relevance: In this randomized clinical trial, use of a standardized multimodal care transition intervention targeting higher-risk patients did not significantly decrease the risks of 30-day postdischarge unplanned readmission or death; it demonstrated the difficulties in preventing hospital readmissions, even when multimodal interventions specifically target higher-risk patients.
Trial registration: ClinicalTrials.gov Identifier: NCT03496896.
Conflict of interest statement
Figures


Comment in
-
The Disappointing Impact of Interventions to Prevent Hospital Readmissions.JAMA Intern Med. 2023 Jul 1;183(7):668-669. doi: 10.1001/jamainternmed.2023.0804. JAMA Intern Med. 2023. PMID: 37126339 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
