

Lung Ultrasound to Assess Pulmonary Congestion in Patients with Acute Exacerbation of COPD
- PMID: 37128214
- PMCID: PMC10148645
- DOI: 10.2147/COPD.S396855
Lung Ultrasound to Assess Pulmonary Congestion in Patients with Acute Exacerbation of COPD
Abstract
Purpose: Heart failure (HF) often coexists with chronic obstructive pulmonary disease (COPD) and is associated with worse outcomes. We aimed to assess the feasibility of detecting vertical artifacts (B-lines) on lung ultrasound (LUS) to identify concurrent HF in patients hospitalized with acute exacerbation of COPD (AECOPD). Second, we wanted to assess the association between B-lines and the risk of rehospitalization for AECOPD or death.
Patients and methods: In a prospective cohort study, 123 patients with AECOPD underwent 8-zone bedside LUS within 24h after admission. A positive LUS was defined by ≥3 B-lines in ≥2 zones bilaterally. The ability to detect concurrent HF (adjudicated by a cardiologist committee) and association with events were evaluated by logistic- and Cox regression models.
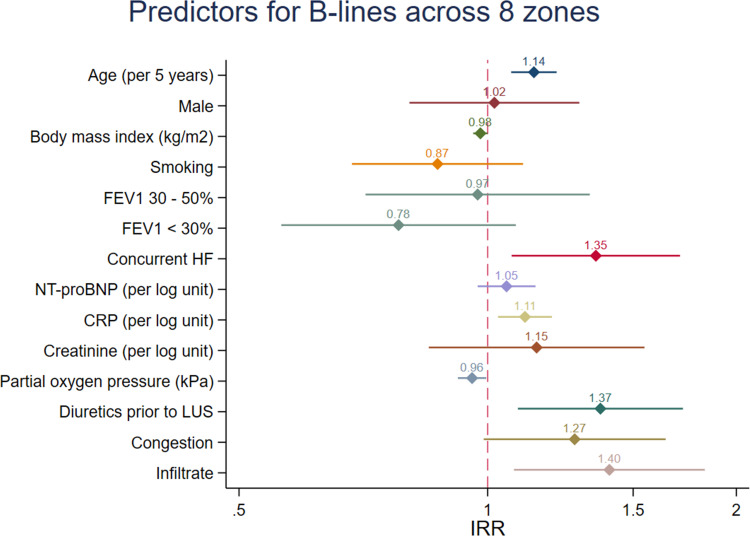
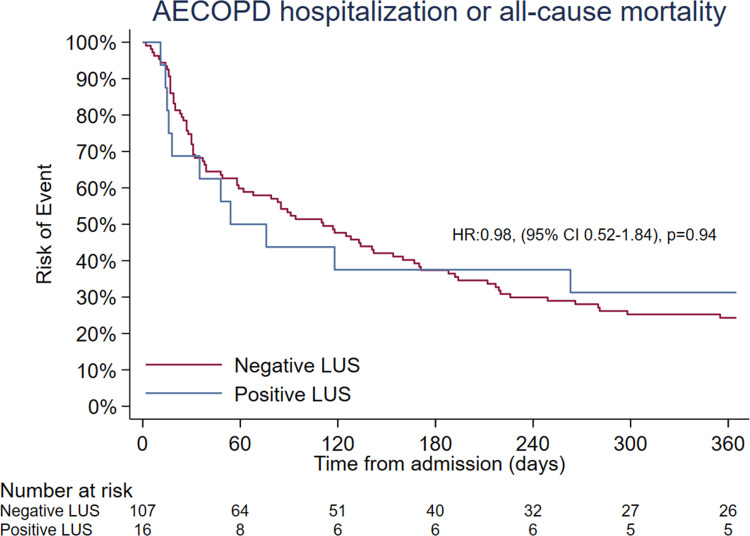
Results: Forty-eight of 123 patients with AECOPD (age 75±9 years, 57[46%] men) had concurrent HF. Sixteen (13%) patients had positive LUS, and the prevalence of positive LUS was similar between patients with and without concurrent HF (8[17%] vs 8[11%], respectively, p=0.34). The number of B-lines was higher in concurrent HF: median 10(IQR 6-16) vs 7(IQR 5-12), p=0.03. The sensitivity and specificity for a positive LUS to detect concurrent HF were 17% and 89%, respectively. Positive LUS was not associated with rehospitalization and mortality: Adjusted HR: 0.93(0.49-1.75), p=0.81.
Conclusion: LUS did not detect concurrent HF or predict risk in patients with AECOPD.
Keywords: B-lines; acute exacerbations; chronic obstructive pulmonary disease; heart failure; lung ultrasound; pulmonary congestion.
© 2023 Johannessen et al.
Conflict of interest statement
Dr. Johannessen has received grants from the Norwegian Society of Pulmonary Physicians, The Norwegian Society for Ultrasound in General Practice, and Astra-Zeneca via the Norwegian Society of Pulmonary Physicians. Dr. Einvik has received grants from the Norwegian Society of Pulmonary Physicians outside of the submitted work. Dr. Myhre is supported by research grants from the South-Eastern Norway Regional Health Authority and has served on advisory boards and consulted for Amarin, AmGen, AstraZeneca, Bayer, Boehringer-Ingelheim, Novartis and Novo Nordisk outside of the submitted work. All other authors report no conflicts of interest in this work.
Figures

Similar articles
-
Value of Lung Ultrasound Sonography B-Lines Quantification as a Marker of Heart Failure in COPD Exacerbation.Int J Chron Obstruct Pulmon Dis. 2024 Aug 1;19:1767-1774. doi: 10.2147/COPD.S447819. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39108664 Free PMC article.
-
Pulmonary congestion evaluated by lung ultrasound predicts decompensation in heart failure outpatients.Int J Cardiol. 2017 Aug 1;240:271-278. doi: 10.1016/j.ijcard.2017.02.150. Int J Cardiol. 2017. PMID: 28606680
-
Detection and prognostic value of pulmonary congestion by lung ultrasound in ambulatory heart failure patients.Eur Heart J. 2016 Apr 14;37(15):1244-51. doi: 10.1093/eurheartj/ehv745. Epub 2016 Jan 26. Eur Heart J. 2016. PMID: 26819225 Free PMC article.
-
Utility of lung ultrasound to identify patients at risk of rehospitalization for acute decompensated heart failure.Curr Probl Cardiol. 2025 Apr;50(4):103002. doi: 10.1016/j.cpcardiol.2025.103002. Epub 2025 Jan 29. Curr Probl Cardiol. 2025. PMID: 39890047 Review.
-
A practical guide to the lung ultrasound for the assessment of congestive heart failure.J Echocardiogr. 2021 Dec;19(4):195-204. doi: 10.1007/s12574-021-00528-7. Epub 2021 Jun 16. J Echocardiogr. 2021. PMID: 34133007 Review.
Cited by
-
Chronic Obstructive Pulmonary Disease and the Management of Cardiopulmonary Risk in the UK: A Systematic Literature Review and Modified Delphi Study.Int J Chron Obstruct Pulmon Dis. 2025 Jun 25;20:2073-2090. doi: 10.2147/COPD.S523865. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40585423 Free PMC article.
-
Lack of Evidence Regarding Markers Identifying Acute Heart Failure in Patients with COPD: An AI-Supported Systematic Review.Int J Chron Obstruct Pulmon Dis. 2024 Feb 23;19:531-541. doi: 10.2147/COPD.S437899. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 38414719 Free PMC article.
-
The Complex Relationship Between Heart Failure and Chronic Obstructive Pulmonary Disease: A Comprehensive Review.J Clin Med. 2025 Jul 6;14(13):4774. doi: 10.3390/jcm14134774. J Clin Med. 2025. PMID: 40649150 Free PMC article. Review.
-
A machine learning-based lung ultrasound algorithm for the diagnosis of acute heart failure.Intern Emerg Med. 2024 Nov;19(8):2309-2318. doi: 10.1007/s11739-024-03627-2. Epub 2024 May 23. Intern Emerg Med. 2024. PMID: 38780749
-
Value of Lung Ultrasound Sonography B-Lines Quantification as a Marker of Heart Failure in COPD Exacerbation.Int J Chron Obstruct Pulmon Dis. 2024 Aug 1;19:1767-1774. doi: 10.2147/COPD.S447819. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39108664 Free PMC article.
References
-
- Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Res Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X - DOI - PMC - PubMed
-
- Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020;5:1–6.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
