

Comparison of High-Flow Nasal Cannula Versus Conventional Oxygen Therapy After Extubation in Children Undergoing Cardiac Surgery: A Meta-analysis
- PMID: 37128521
- PMCID: PMC10148723
- DOI: 10.7759/cureus.36922
Comparison of High-Flow Nasal Cannula Versus Conventional Oxygen Therapy After Extubation in Children Undergoing Cardiac Surgery: A Meta-analysis
Abstract
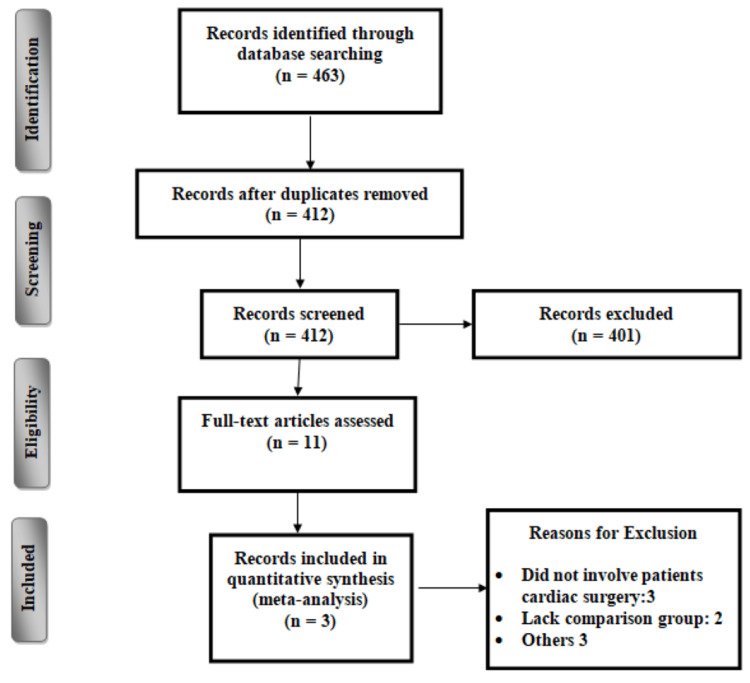
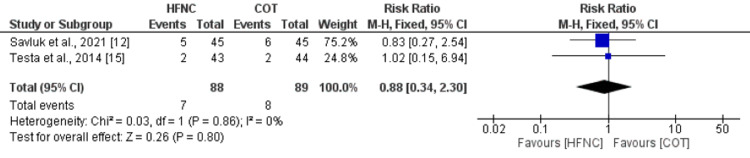
This meta-analysis aims to compare high-flow nasal cannula (HFNC) and conventional oxygen therapy (COT) post-extubation in pediatric cardiac surgical patients. The present meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two authors independently searched three electronic databases including PubMed, Embase, and the Cochrane Library to identify relevant articles published in English from inception to February 2023. Searching was conducted using keywords and medical subject headings (MeSH), which included "conventional oxygen therapy," "high-flow nasal cannula," "extubation," "pediatrics," and "cardiac surgery." Our primary outcome was extubation failure defined as the need for reintubation within 24 to 72 hours after planned extubation. Secondary outcomes assessed in this meta-analysis included partial pressure of arterial oxygen (PaO2), partial pressure of arterial carbon dioxide (PaCO2), and the ratio of PaO2 and FiO2 (fraction of inspired oxygen). A total of three studies were included in the meta-analysis, with a total of 227 patients. No significant difference was found between the two groups (the HFNC group and the COT group) in terms of reintubation (RR: 0.88, 95% CI: 0.34, 2.30, p-value: 0.80). Pooled meta-analysis showed that PaO2 was significantly greater in patients receiving HFNC at six hours (MD: 33.73, 95% CI: 18.33, 49.14, p-value<0.001), at 12 hours (MD: 44.90, 95% CI: 28.59, 61.22, p-value<0.001) and at 24 hours (MD: 43.53, 95% CI: 29.16, 57.91, p-value<0.001) of extubation. PaCO2 was significantly lower in patients receiving HFNC at six hours (MD: -5.40, 95% CI: -7.94, -2.85, p-value<0.001) and at 12 hours (MD: -5.93, 95% CI: -9.78, -2.09, p-value<0.001) of extubation. However, no significant difference was reported between the two groups after 24 hours of extubation (MD: -0.84, 95% CI: -9.04, 7.37, p-value: 0.84) and PaO2/FiO2 was significantly greater in patients receiving HFNC at six hours (MD: 64.14, 95% CI: 36.10, 92.17, p-value<0.001), at 12 hours (MD: 70.73, 95% CI: 20.46, 121.01, p-value<0.001) and at 24 hours (MD: 82.18, 95% CI: 50.03, 114.32, p-value<0.001) of intubation. In conclusion, the meta-analysis revealed that compared with COT, HFNC significantly increased PaO2 and the ratio of PaO2 to FiO2, and decreased PaCO2. No significant differences were observed in the rate of reintubation between the two groups. This is the first meta-analysis comparing HFNC and COT in pediatric cardiac surgical patients.
Keywords: cardiac surgery; children; conventional oxygen therapy; high flow nasal cannula; meta-analysis.
Copyright © 2023, Karedath et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Weaning from ventilatory support. Epstein SK. Curr Opin Crit Care. 2009;15:36–43. - PubMed
-
- The role of noninvasive ventilation in the ventilator discontinuation process. Hess DR. Respir Care. 2012;57:1619–1625. - PubMed
-
- Evolution of mortality over time in patients receiving mechanical ventilation. Esteban A, Frutos-Vivar F, Muriel A, et al. Am J Respir Crit Care Med. 2013;188:220–230. - PubMed
-
- Heated, humidified high-flow nasal cannula therapy: yet another way to deliver continuous positive airway pressure? Kubicka ZJ, Limauro J, Darnall RA. Pediatrics. 2008;121:82–88. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous