

Systematic review and meta-analysis of mesenchymal stromal/stem cells as strategical means for the treatment of COVID-19
- PMID: 37128999
- PMCID: PMC10140776
- DOI: 10.1177/17534666231158276
Systematic review and meta-analysis of mesenchymal stromal/stem cells as strategical means for the treatment of COVID-19
Abstract
Background: In coronavirus disease 2019 (COVID-19) patients, elevated levels of inflammatory cytokines from over stimulation of immune cells have become a concern due to the potential outburst of cytokine storm that damages the tissues and organs, especially the lungs. This leads to the manifestation of COVID-19 symptoms, such as pneumonia, acute respiratory distress syndrome (ARDS), multiple organ failure, and eventually death. Mesenchymal stromal/stem cells (MSCs) are currently one of hopeful approaches in treating COVID-19 considering its anti-inflammatory and immunomodulatory functions. On that account, the number of clinical trials concerning the use of MSCs for COVID-19 has been increasing. However, the number of systematic reviews and meta-analysis that specifically discuss its potential as treatment for the disease is still lacking. Therefore, this review will assess the safety and efficacy of MSC administration in COVID-19 patients.
Objectives: To pool evidence on the safety and efficacy of MSCs in treating COVID-19 by observing MSC-related adverse effects as well as evaluating its effects in reducing inflammatory response and improving pulmonary function.
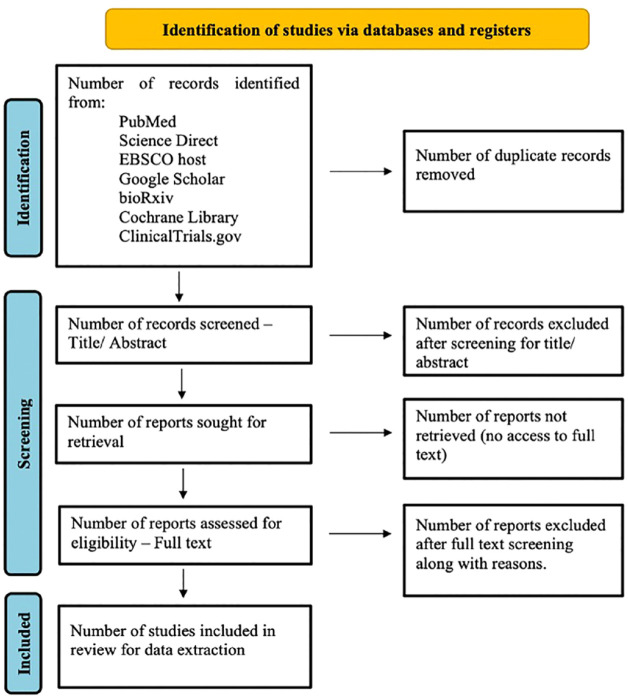
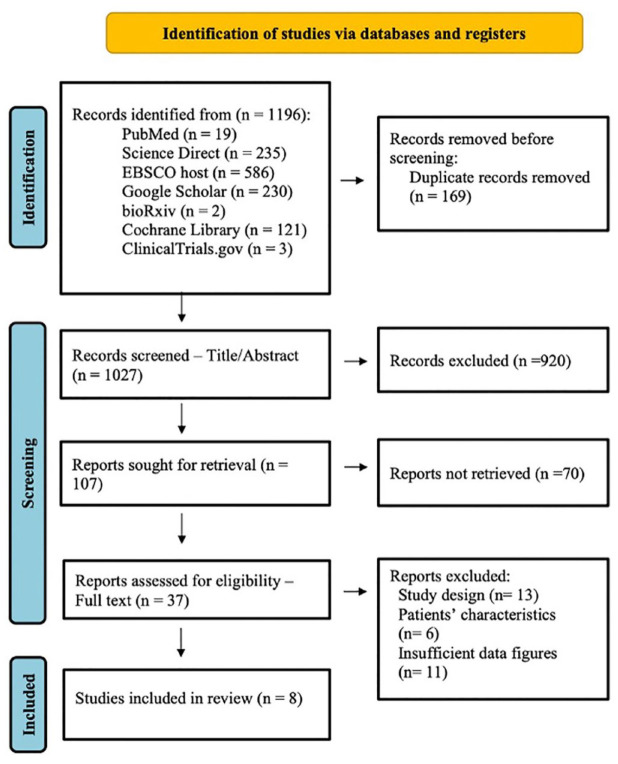
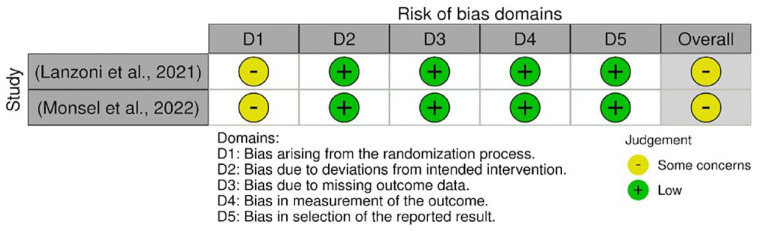
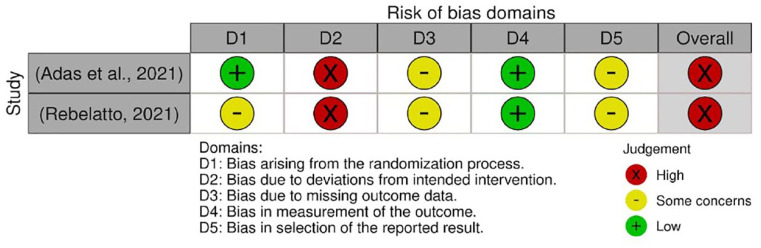
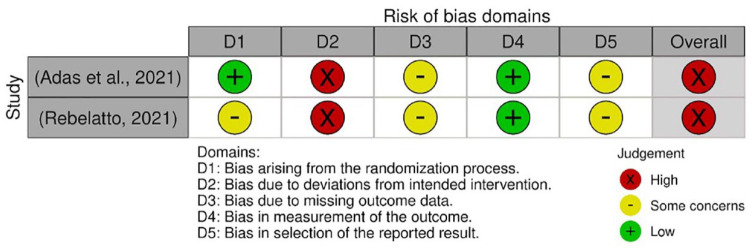
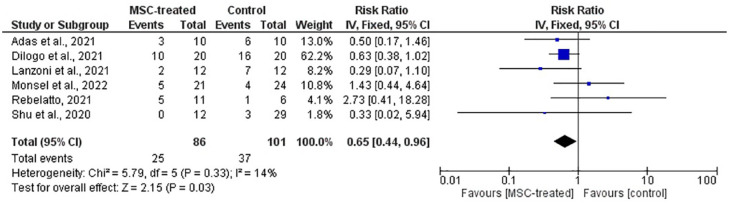
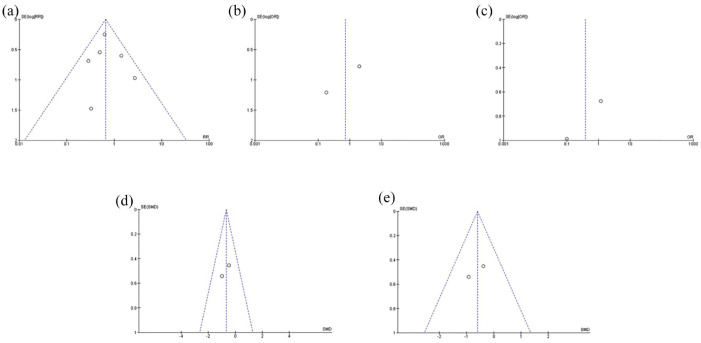
Data sources and methods: Following literature search across six databases and one trial register, full-text retrieval, and screening against eligibility criteria, only eight studies were included for data extraction. All eight studies evaluated the use of umbilical cord-derived mesenchymal stromal/stem cell (UC-MSC), infused intravenously. Of these eight studies, six studies were included in meta-analysis on the incidence of mortality, adverse events (AEs), and serious adverse events (SAEs), and the levels of C-reactive protein (CRP) and interleukin (IL)-6. Meta-analysis on pulmonary function was not performed due to insufficient data.
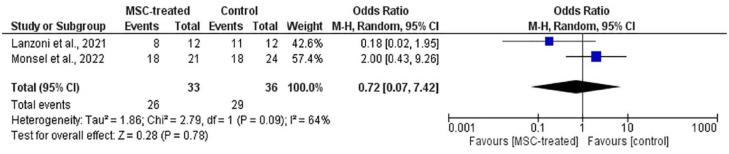
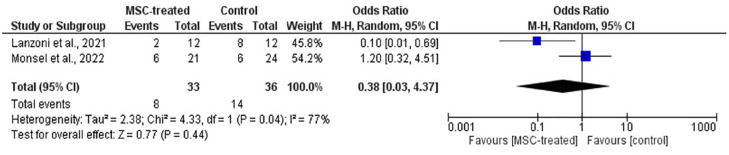
Results: MSC-treated group showed significantly lower risk of mortality than the control group (p = 0.03). No statistical significance was observed on the incidence of AEs (p = 0.78) and SAEs (p = 0.44), and the levels of CRP (p = 0.06) and IL-6 (p = 0.09).
Conclusion: MSCs were safe for use, with lower risk of mortality and no association with AEs. Regarding efficacy, descriptive analysis showed indications of improvement on the inflammatory reaction, lung clearance, and oxygenation status despite the lack of statistical significance in meta-analysis of CRP and IL-6. Nevertheless, more studies are needed for affirmation.
Registration: This systematic review and meta-analysis was registered on the PROSPERO database (no. CRD42022307730).
Keywords: COVID-19; SARS-CoV-2; mesenchymal stromal/stem cells.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
