

2023 Update on European Atherosclerosis Society Consensus Statement on Homozygous Familial Hypercholesterolaemia: new treatments and clinical guidance
- PMID: 37130090
- PMCID: PMC10314327
- DOI: 10.1093/eurheartj/ehad197
2023 Update on European Atherosclerosis Society Consensus Statement on Homozygous Familial Hypercholesterolaemia: new treatments and clinical guidance
Abstract
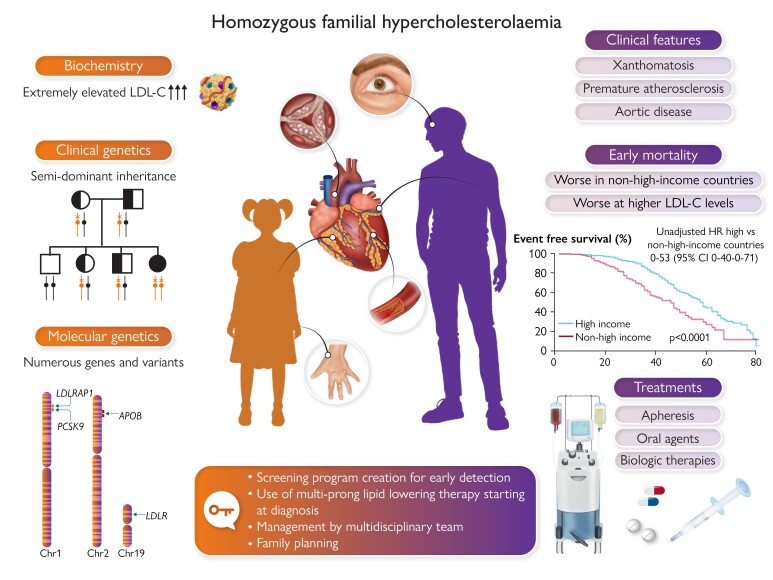
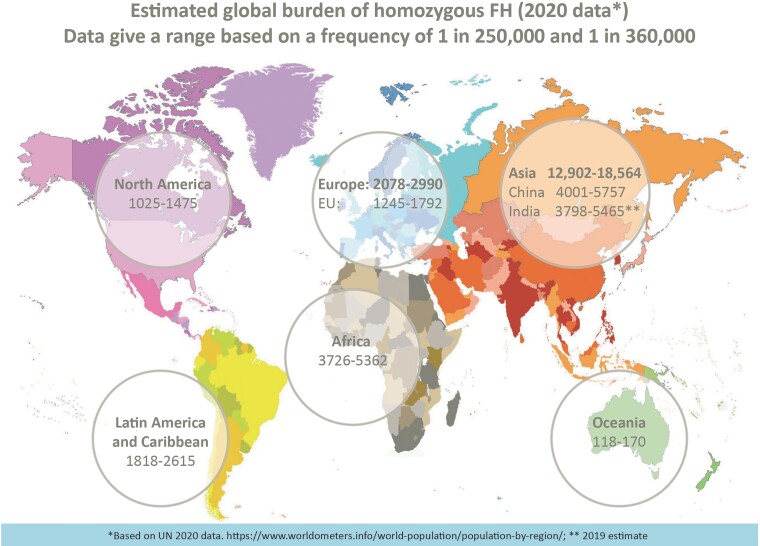
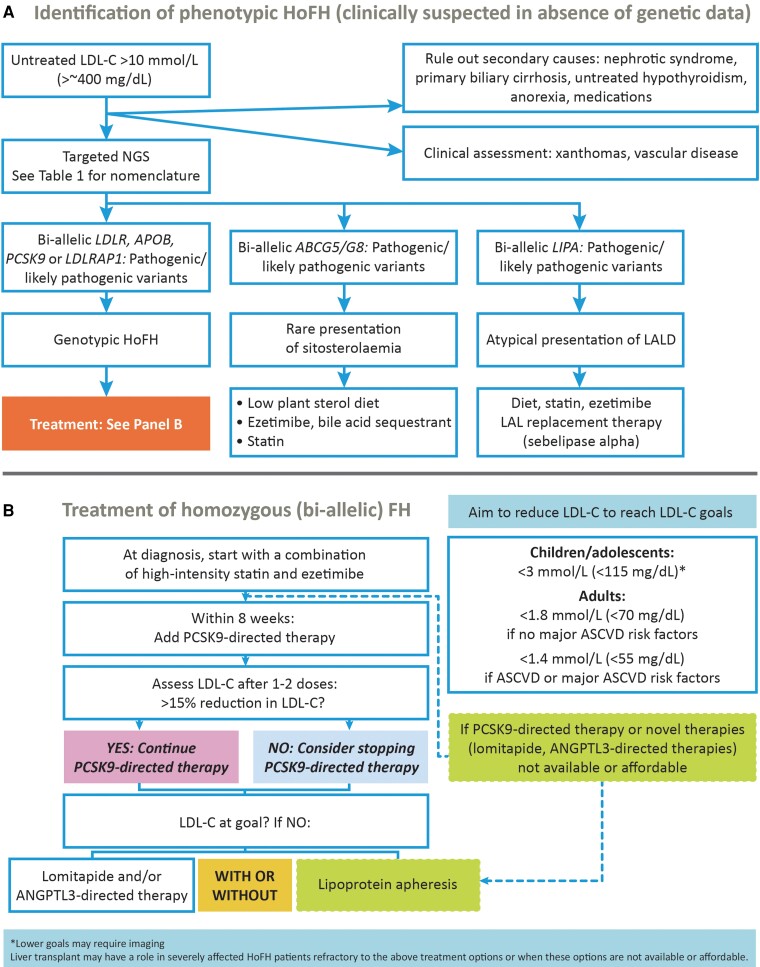
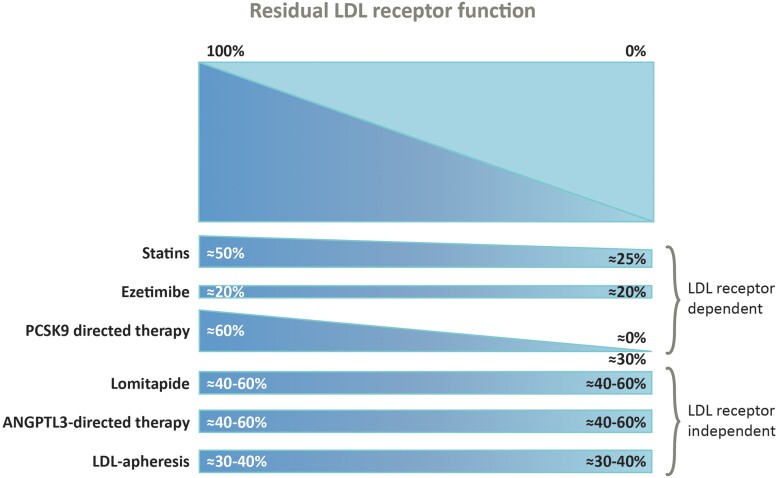
This 2023 statement updates clinical guidance for homozygous familial hypercholesterolaemia (HoFH), explains the genetic complexity, and provides pragmatic recommendations to address inequities in HoFH care worldwide. Key strengths include updated criteria for the clinical diagnosis of HoFH and the recommendation to prioritize phenotypic features over genotype. Thus, a low-density lipoprotein cholesterol (LDL-C) >10 mmol/L (>400 mg/dL) is suggestive of HoFH and warrants further evaluation. The statement also provides state-of-the art discussion and guidance to clinicians for interpreting the results of genetic testing and for family planning and pregnancy. Therapeutic decisions are based on the LDL-C level. Combination LDL-C-lowering therapy-both pharmacologic intervention and lipoprotein apheresis (LA)-is foundational. Addition of novel, efficacious therapies (i.e. inhibitors of proprotein convertase subtilisin/kexin type 9, followed by evinacumab and/or lomitapide) offers potential to attain LDL-C goal or reduce the need for LA. To improve HoFH care around the world, the statement recommends the creation of national screening programmes, education to improve awareness, and management guidelines that account for the local realities of care, including access to specialist centres, treatments, and cost. This updated statement provides guidance that is crucial to early diagnosis, better care, and improved cardiovascular health for patients with HoFH worldwide.
Keywords: Clinical guidance; Diagnosis; Genetics; Homozygous familial hypercholesterolaemia; Treatment; Women.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest Potential conflicts of interest outside the submitted work are summarized as follows. The following authors report participation in trials; receipt of fellowships, or grants for travel, research or staffing support; and/or personal honoraria for consultancy or lectures/speaker’s bureau from: Abbott (K.A.-R., M.K., K.K.R., R.D.S., L.S.T.); Abdi-Ibrahim (M.K., L.S.T.); Acasti (D.G., R.A.H.); Ache (R.D.S.); Actelion (L.S.T.); Aegerion (M.A., E.B., D.G., M.H.-S.); Akcea (M.A., E.B., A.L.C., D.G., R.A.H., K.G.P.); Alexion Pharma France (E.B.); Alfasigma (M.A.); Amarin (M.A., M.Av., A.L.C., L.M.); Amgen (M.A., M.Av., E.B., T.F., D.G., M.H.-S., R.A.H., M.K., L.M., K.G.P., F.J.R., K.K.R., R.D.S., L.S.T., G.F.W., A.W.); Amryt (M.A., M.Av., MC, M.K., L.M., J.E.R.v.L., R.D.S., A.W.); Arrowhead (R.A.H., G.F.W.); Ascent Development (M.H.-S.); Astellas (M.H.-S.); AstraZeneca (A.L.C., D.G., M.K., K.K.R., R.D.S., G.F.W.); Bayer (M.K., L.S.T.); Biolab (R.D.S.); Boehringer Ingelheim (D.G., M.H.-S., K.K.R.); Cerenis (D.G.); CRISPR Therapeutics (K.K.R.); Daiichi-Sankyo (M.Av., E.B., A.L.C., M.H.-S., M.K., L.M., K.G.P., K.K.R., L.S.T.); Dalcor Pharma (D.G.); Danone (E.B.); Deva (M.K.); Esperion (A.L.C., D.G., K.K.R., R.D.S., G.F.W.); Gemphire (D.G.); Genfit (E.B.); Genzyme (A.L.C.); Getz Pharma (R.D.S.); GlaxoSmithKline (D.G.); HDL Therapeutics (D.G.); HLS Therapeutics (R.A.H.); Ionis Pharmaceuticals (E.B., A.L.C., D.G., M.K.); Ironwood (D.G.); Jansen (M.K.); Kowa (A.L.C., D.G., M.H.-S., K.K.R., R.D.S.); LIB Therapeutics (R.A.H., M.K., F.J.R.); Libbs (R.D.S.); Eli Lilly/Lilly (A.L.C., D.G., M.K., K.K.R.); Medpace (M.H.-S., M.K.); Menarini (A.L.C.); Merck (A.L.C., M.K., R.D.S., L.S.T.); MSD (E.B., M.H.-S., K.G.P.); Mylan (M.A., E.B., A.L.C.); Nestlé (D.G.); New Amsterdam (K.K.R.); Novartis (K.A.-R., M.A., M.Av., E.B., A.L.C., T.F., D.G., M.H.-S., R.A.H., M.K., L.M., K.G.P., K.K.R., J.E.R.v.L., F.J.R., R.D.S., L.S.T., G.F.W., A.W.); NovoNordisk (M.K., K.K.R., R.D.S., L.S.T.); Pfizer (M.A., A.L.C., D.G., R.A.H., M.K., K.K.R., R.D.S., L.S.T., G.F.W.); PTC (R.D.S.); Recordati (A.L.C., M.H.-S., M.K., L.S.T.); Regeneron (M.A., A.L.C., MC, D.G., R.A.H., K.G.P., F.J.R., K.K.R., A.W.); REGENXBIO (M.C.); Resverlogix (K.K.R.); Sandoz (A.L.C.); Sanofi (K.A.-R., M.A., A.L.C., T.F., D.G., M.H.-S., R.A.H., M.K., L.M., K.G.P., F.J.R., K.K.R., R.D.S., L.S.T., G.F.W.); Sanofi/Genzyme (M.Av.); Sanofi-Regeneron (E.B.); SCIBE Therapeutics (K.K.R.); Servier (E.B., L.M., L.S.T.); Sigma Tau (A.L.C.); Silence Therapeutics (E.B., K.G.P., K.K.R., G.F.W., A.W.); Sobi Takeda (M.Av.); The Medicine Company (D.G., M.H.-S.); Ultragenyx (R.A.H.); UniQure (D.G.); and Vaxxinity (K.K.R.). ESG Stroes reports honoraria for lectures/advisory board R.D.S. paid to his institution from Amarin, Amgen, Daiichi-Sankyo, Esperion, IONIS/Akcea, Novartis, Novo-Nordisk, and Sanofi-Regeneron. Manuscripts have been published in collaboration with non-academic co-authors by L.S.T. (Fitbit), and G.F.W. (Amgen). T.F. is supported by the project National Institute for Research of Metabolic and Cardiovascular Diseases (Programme EXCELES, ID Project No. LX22NPO5104)—Funded by the European Union—Next Generation EU. D.G. is supported by Canadian Cardiovascular Research Network and the Institut de cardiologie de Montréal. Equity interests are reported by K.K.R. (Cargene Therapeutics and Pemi31 Therapeutics) and J.K.S. (AstraZeneca and GSK). K.K.R. is President of the European Atherosclerosis Society. L.S.T. is Past-President of the European Atherosclerosis Society and an Editorial Board Member, The European Heart Journal. L.C.H. has no disclosures.
Figures
References
-
- Cuchel M, Bruckert E, Ginsberg HN, Raal FJ, Santos RD, Hegele RA, et al. Homozygous familial hypercholesterolaemia: new insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur Heart J 2014;35:2146–2157. 10.1093/eurheartj/ehu274 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
