

Development of a modified Cambridge Multimorbidity Score for use with SNOMED CT: an observational English primary care sentinel network study
- PMID: 37130611
- PMCID: PMC10170523
- DOI: 10.3399/BJGP.2022.0235
Development of a modified Cambridge Multimorbidity Score for use with SNOMED CT: an observational English primary care sentinel network study
Abstract
Background: People with multiple health conditions are more likely to have poorer health outcomes and greater care and service needs; a reliable measure of multimorbidity would inform management strategies and resource allocation.
Aim: To develop and validate a modified version of the Cambridge Multimorbidity Score in an extended age range, using clinical terms that are routinely used in electronic health records across the world (Systematized Nomenclature of Medicine - Clinical Terms, SNOMED CT).
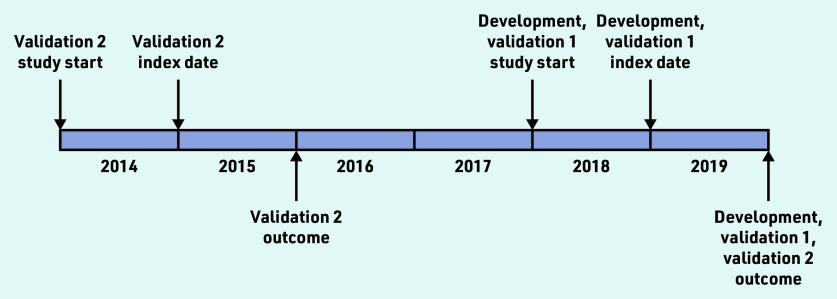
Design and setting: Observational study using diagnosis and prescriptions data from an English primary care sentinel surveillance network between 2014 and 2019.
Method: In this study new variables describing 37 health conditions were curated and the associations modelled between these and 1-year mortality risk using the Cox proportional hazard model in a development dataset (n = 300 000). Two simplified models were then developed - a 20-condition model as per the original Cambridge Multimorbidity Score and a variable reduction model using backward elimination with Akaike information criterion as the stopping criterion. The results were compared and validated for 1-year mortality in a synchronous validation dataset (n = 150 000), and for 1-year and 5-year mortality in an asynchronous validation dataset (n = 150 000).
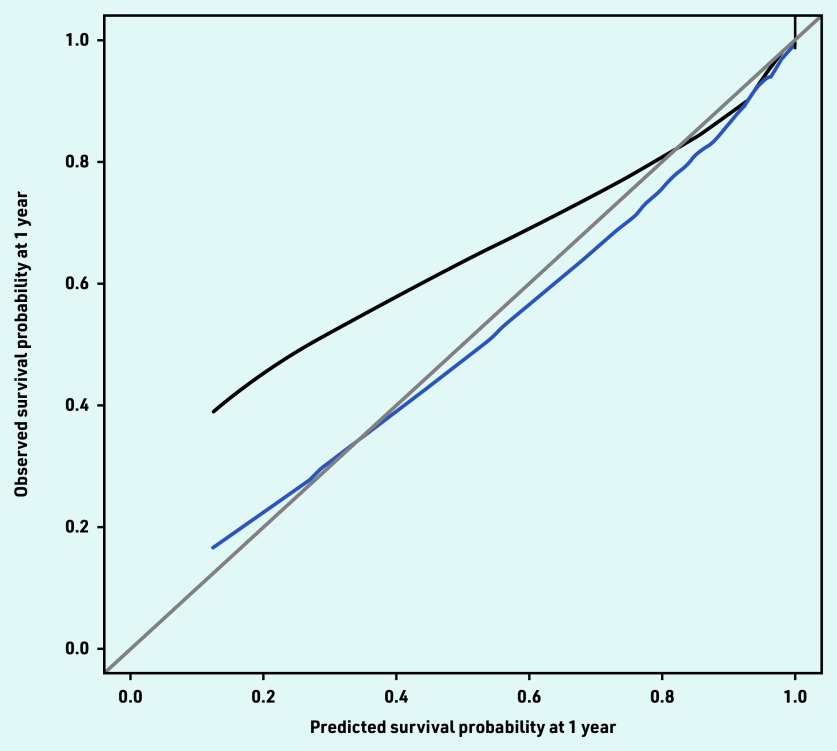
Results: The final variable reduction model retained 21 conditions, and the conditions mostly overlapped with those in the 20-condition model. The model performed similarly to the 37- and 20-condition models, showing high discrimination and good calibration following recalibration.
Conclusion: This modified version of the Cambridge Multimorbidity Score allows reliable estimation using clinical terms that can be applied internationally across multiple healthcare settings.
Keywords: Systematized Nomenclature of Medicine–Clinical Terms; general practice; medical record systems, computerised; mortality; multimorbidity; population surveillance.
© The Authors.
Conflict of interest statement
Simon de Lusignan is Director of the RCGP RSC; he has had grants through his University from AstraZeneca, GSK, Lily, MSD, Sanofi, Seqirus, and Takeda; and has been an advisory board member for AstraZeneca, Sanofi, Seqirus, and Pfizer.
Figures
References
-
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. - PubMed
-
- Elixhauser A, Steiner C, Harris DR, et al. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. - PubMed
-
- Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619. - PubMed
-
- Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004;57(12):1288–1294. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources