

Early intensive mobilization after acute high-risk abdominal surgery: a nonrandomized prospective feasibility trial
- PMID: 37130709
- PMCID: PMC10158751
- DOI: 10.1503/cjs.008722
Early intensive mobilization after acute high-risk abdominal surgery: a nonrandomized prospective feasibility trial
Abstract
Background: Mobilization after emergency abdominal surgery is considered essential to facilitate rehabilitation and reduce postoperative complications. The aim of this study was to evaluate the feasibility of early intensive mobilization after acute high-risk abdominal (AHA) surgery.
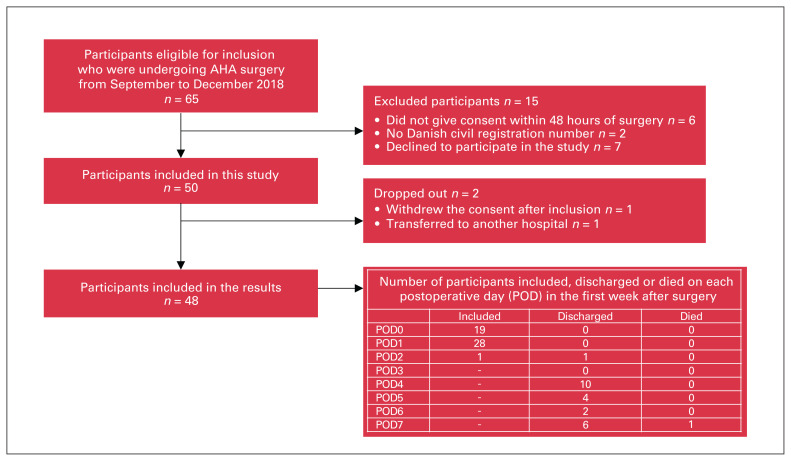
Methods: We conducted a nonrandomized, prospective feasibility trial of consecutive patients after AHA surgery at a university hospital in Denmark. The participants followed a predefined, interdisciplinary protocol for early intensive mobilization during the first 7 postoperative days (PODs) of their hospital admission. We evaluated feasibility in accordance with the percentage of patients who mobilized within 24 hours after surgery, mobilized at least 4 times per day and achieved daily goals of time out of bed and walking distance.
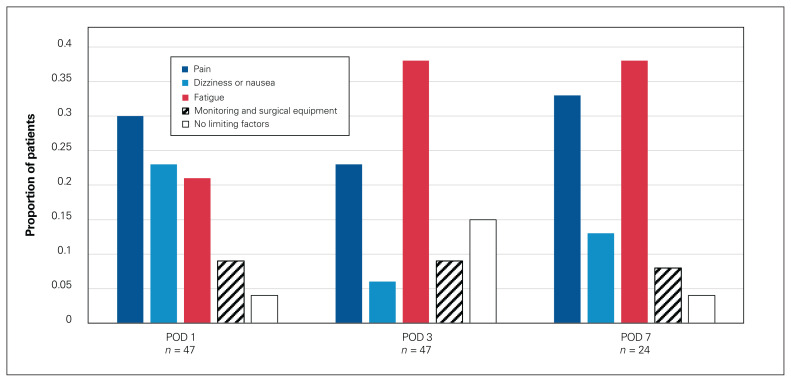
Results: We included 48 patients with a mean age of 61 (standard deviation 17) years (48% female). Within 24 hours after surgery, 92% of the patients were mobilized and 82% or more were mobilized at least 4 times per day over the first 7 PODs. On PODs 1-3, 70%-89% of the participants achieved the daily goals of mobilization; participants still in hospital after POD 3 were less able to achieve the daily goals. Patient reported that the primary factors limiting their level of mobilization were fatigue, pain and dizziness. Participants not mobilized independently on POD 3 (28%) had significantly (p ≤ 0.04) fewer hours out of bed (4 v. 8 h), were less able to achieve the goals of time out of bed (45% v. 95%) and walking distance (62% v. 94%) and had longer hospital stays (14 v. 6 d) than participants mobilized independently on POD 3.
Conclusion: The early intensive mobilization protocol seems feasible for most patients after AHA surgery. For nonindependent patients, however, alternative mobilization strategies and goals should be investigated.
Contexte:: On considère essentiel de mobiliser les malades après une intervention abdominale urgente afin de faciliter leur réadaptation et de réduire le risque de complications postopératoires. Le but de cette étude était d’évaluer la faisabilité d’une mobilisation intensive précoce après une chirurgie abdominale urgente à haut risque.
Méthodes:: Nous avons procédé à un essai de faisabilité prospectif non randomisé auprès de malades consécutifs ayant subi une chirurgie abdominale urgente à haut risque dans un centre hospitalier universitaire du Danemark. Nous avons appliqué un protocole interdisciplinaire prédéfini pour une mobilisation intensive précoce pendant les 7 premiers jours postopératoires. Nous avons évalué la faisabilité en fonction du pourcentage de malades ayant été mobilisés au cours de 24 premières heures suivant la chirurgie, ayant été mobilisés au moins 4 fois par jour et ayant atteint les objectifs quotidiens fixés pour le temps passé hors du lit et une distance franchie en marchant.
Résultats:: Nous avons inclus 48 malades âgés en moyenne de 61 ans (écart-type 17; 48 % de sexe féminin). Dans les 24 heures suivant la chirurgie, 92 % des malades ont été mobilisés et 82 % ou plus l’ont été au moins 4 fois par jour au cours des 7 premiers jours postopératoires. Aux jours postopératoires 1–3, 70 %–89 % des participants ont atteint les objectifs quotidiens de mobilisation; les malades encore hospitalisés 3 jours après l’intervention étaient moins en mesure d’atteindre les objectifs quotidiens. Aux dires des malades, les principaux facteurs ayant limité leur mobilisation étaient la fatigue, la douleur et les étourdissements. Les participants qui n’avaient pas bénéficié de l’intervention de mobilisation autonome au 3e jour postopératoire (28 %) avaient passé une nombre d’heures significativement moindre (p ≤ 0,04) hors du lit (4 c. 8 h), étaient moins aptes à atteindre les objectifs en terme de temps passé hors du lit (45 % c. 95 %) et de distance parcourue en marchant (62 % c. 94 %), et leur séjour hospitalier a été plus long (14 c. 6 j) comparativement aux malades soumis à l’intervention de mobilisation autonome au 3e jour postopératoire.
Conclusion:: Le protocole de mobilisation intensive précoce semble faisable pour la plupart des malades après une chirurgie abdominale urgente à haut risque. Pour les malades non autonomes, toutefois, il faudra explorer d’autres stratégies de mobilisation et fixer d’autres objectifs.
© 2023 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Tengberg LT, Cihoric M, Foss NB, et al. . Complications after emergency laparotomy beyond the immediate postoperative period — a retrospective, observational cohort study of 1139 patients. Anaesthesia 2017;72:309–16. - PubMed
-
- Perilli V, Aceto P, Ancona P, et al. . Role of surgical setting and patients-related factors in predicting the occurrence of postoperative pulmonary complications after abdominal surgery. Eur Rev Med Pharmacol Sci 2018;22:547–50. - PubMed
-
- Tengberg LT, Bay-Nielsen M, Bisgaard T, et al. . Multidisciplinary perioperative protocol in patients undergoing acute high-risk abdominal surgery. Br J Surg 2017;104:463–71. - PubMed
-
- Foss NB, Kehlet H. Challenges in optimising recovery after emergency laparotomy. Anaesthesia 2020;75:e83–9. - PubMed
-
- Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg 2017;152:292–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical