

Potential pharmacological confounders in the setting of death determined by neurologic criteria: a narrative review
- PMID: 37131030
- PMCID: PMC10202973
- DOI: 10.1007/s12630-023-02415-4
Potential pharmacological confounders in the setting of death determined by neurologic criteria: a narrative review
Abstract
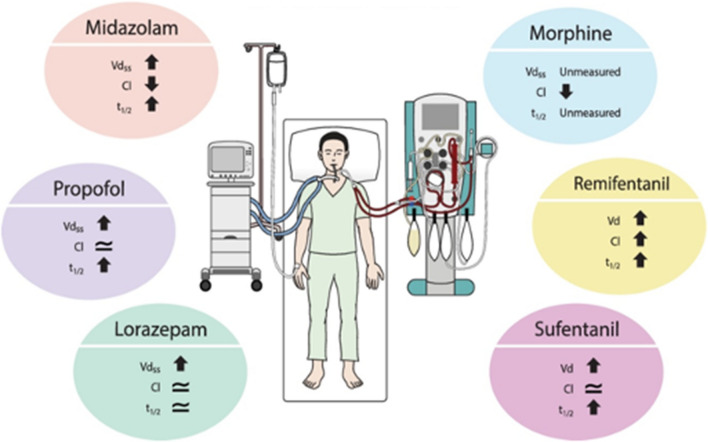
Guidelines for the determination of death by neurologic criteria (DNC) require an absence of confounding factors if clinical examination alone is to be used. Drugs that depress the central nervous system suppress neurologic responses and spontaneous breathing and must be excluded or reversed prior to proceeding. If these confounding factors cannot be eliminated, ancillary testing is required. These drugs may be present after being administered as part of the treatment of critically ill patients. While measurement of serum drug concentrations can help guide the timing of assessments for DNC, they are not always available or feasible. In this article, we review sedative and opioid drugs that may confound DNC, along with pharmacokinetic factors that govern the duration of drug action. Pharmacokinetic parameters including a context-sensitive half-life of sedatives and opioids are highly variable in critically ill patients because of the multitude of clinical variables and conditions that can affect drug distribution and clearance. Patient-, disease-, and treatment-related factors that influence the distribution and clearance of these drugs are discussed including end organ function, age, obesity, hyperdynamic states, augmented renal clearance, fluid balance, hypothermia, and the role of prolonged drug infusions in critically ill patients. In these contexts, it is often difficult to predict how long after drug discontinuation the confounding effects will take to dissipate. We propose a conservative framework for evaluating when or if DNC can be determined by clinical criteria alone. When pharmacologic confounders cannot be reversed, or doing so is not feasible, ancillary testing to confirm the absence of brain blood flow should be obtained.
RéSUMé: Les lignes directrices pour la détermination du décès selon des critères neurologiques (DCN) exigent une absence de facteurs confondants si l’examen clinique seul doit être utilisé. Les médicaments qui dépriment le système nerveux central suppriment les réponses neurologiques et la respiration spontanée et doivent être exclus ou neutralisés avant de procéder. Si ces facteurs confondants ne peuvent être éliminés, un examen auxiliaire est nécessaire. Ces médicaments peuvent être présents après avoir été administrés dans le cadre du traitement de patients en état critique. Bien que la mesure des concentrations sériques de médicaments puisse guider l’horaire des évaluations pour un DCN, ces mesures ne sont pas toujours disponibles ou réalisables. Dans cet article, nous passons en revue les médicaments sédatifs et opioïdes qui peuvent confondre un DCN, ainsi que les facteurs pharmacocinétiques qui régissent la durée d’action de ces médicaments. Les paramètres pharmacocinétiques, y compris une demi-vie des sédatifs et des opioïdes sensible au contexte, sont très variables chez les patients gravement malades en raison de la multitude de variables cliniques et de conditions qui peuvent affecter la diffusion et l’élimination des médicaments. Les facteurs liés au patient, à la maladie et au traitement qui influencent la diffusion et l’élimination de ces médicaments sont discutés, notamment la fonction des organes cibles, l’âge, l’obésité, les états hyperdynamiques, l’augmentation de la clairance rénale, l’équilibre liquidien, l’hypothermie et le rôle des perfusions prolongées de médicaments chez les patients gravement malades. Dans ces contextes, il est souvent difficile de prédire combien de temps après l’arrêt du médicament les effets confusionnels prendront pour se dissiper. Nous proposons un cadre conservateur pour évaluer quand ou si un DCN peut être déterminé selon des critères cliniques uniquement. Lorsque les facteurs confondants pharmacologiques ne peuvent pas être neutralisés, ou que cela n’est pas possible, un examen auxiliaire pour confirmer l’absence de circulation sanguine cérébrale doit être réalisé.
Keywords: death determination by neurologic criteria; drug confounders; opioids; pharmacokinetics sedatives.
© 2023. The Author(s).
Conflict of interest statement
No author has conflicts of interest to disclose.
Figures

Similar articles
-
Determination of Brain Death/Death by Neurologic Criteria: The World Brain Death Project.JAMA. 2020 Sep 15;324(11):1078-1097. doi: 10.1001/jama.2020.11586. JAMA. 2020. PMID: 32761206
-
Sedation for the critically ill neurologic patient.Crit Care Med. 1995 Dec;23(12):2038-53. doi: 10.1097/00003246-199512000-00013. Crit Care Med. 1995. PMID: 7497727 Review.
-
Altered Pharmacokinetics in Prolonged Infusions of Sedatives and Analgesics Among Adult Critically Ill Patients: A Systematic Review.Clin Ther. 2018 Sep;40(9):1598-1615.e2. doi: 10.1016/j.clinthera.2018.07.021. Epub 2018 Aug 31. Clin Ther. 2018. PMID: 30173953
-
Optimal intravenous dosing strategies for sedatives and analgesics in the intensive care unit.Crit Care Clin. 1995 Oct;11(4):827-47. Crit Care Clin. 1995. PMID: 8535981 Review.
-
Effects of sedatives and opioids on trigger and cycling asynchronies throughout mechanical ventilation: an observational study in a large dataset from critically ill patients.Crit Care. 2019 Jul 5;23(1):245. doi: 10.1186/s13054-019-2531-5. Crit Care. 2019. PMID: 31277722 Free PMC article.
Cited by
-
Distribution and elimination kinetics of midazolam and metabolites after post-resuscitation care: a prospective observational study.Sci Rep. 2024 Feb 25;14(1):4574. doi: 10.1038/s41598-024-54968-z. Sci Rep. 2024. PMID: 38403792 Free PMC article.
-
Pharmacokinetics of Opioid Infusions in the Adult Intensive Care Unit Setting-A Systematic Review.Clin Pharmacokinet. 2025 Mar;64(3):323-334. doi: 10.1007/s40262-025-01490-8. Epub 2025 Mar 1. Clin Pharmacokinet. 2025. PMID: 40025366
References
-
- Wijdicks EF, Varelas PN, Gronseth GS, Greer DM, American Academy of Neurology. Evidence-based guideline update: determining brain death in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010; 74: 1911–8. 10.1212/wnl.0b013e3181e242a8 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
