

A machine-learning-based prediction of non-home discharge among acute heart failure patients
- PMID: 37131097
- PMCID: PMC10955024
- DOI: 10.1007/s00392-023-02209-0
A machine-learning-based prediction of non-home discharge among acute heart failure patients
Abstract
Background: Scarce data on factors related to discharge disposition in patients hospitalized for acute heart failure (AHF) were available, and we sought to develop a parsimonious and simple predictive model for non-home discharge via machine learning.
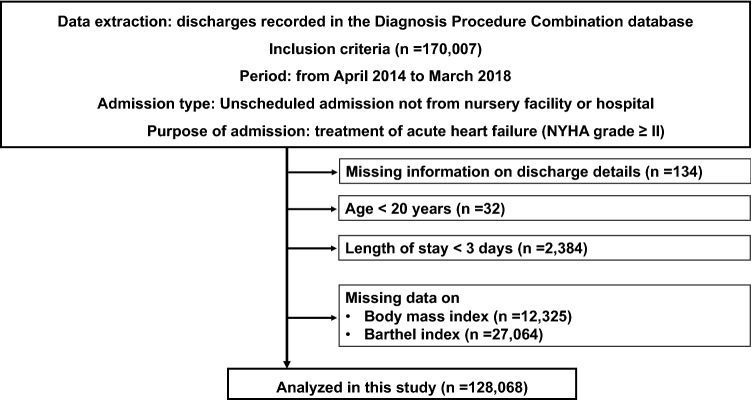
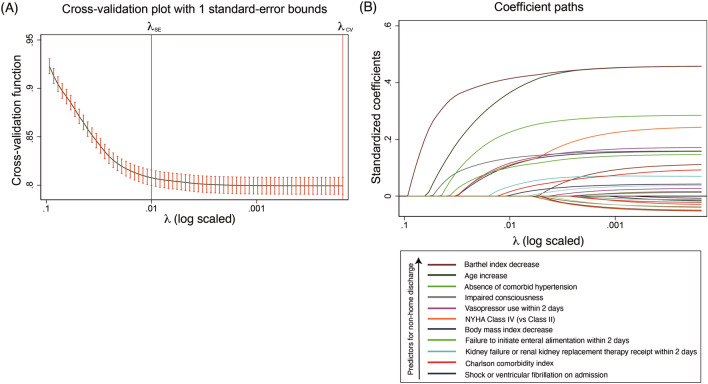
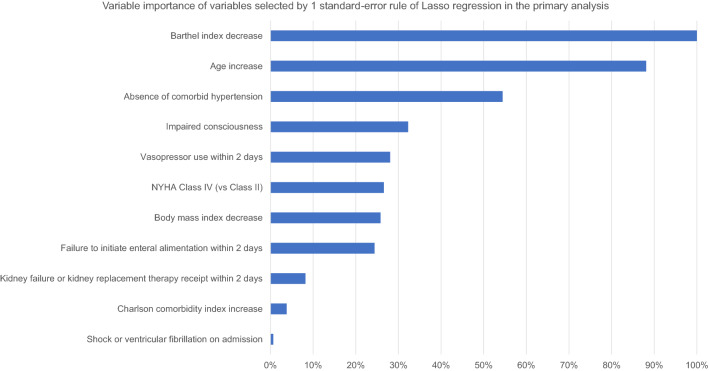
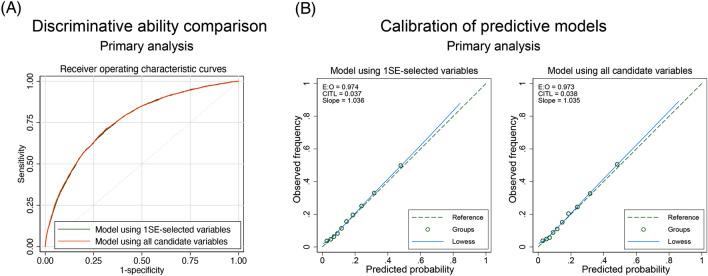
Methods: This observational cohort study using a Japanese national database included 128,068 patients admitted from home for AHF between April 2014 and March 2018. The candidate predictors for non-home discharge were patient demographics, comorbidities, and treatment performed within 2 days after hospital admission. We used 80% of the population to develop a model using all 26 candidate variables and using the variable selected by 1 standard-error rule of Lasso regression, which enhances interpretability, and 20% to validate the predictive ability.
Results: We analyzed 128,068 patients, and 22,330 patients were not discharged to home; 7,879 underwent in-hospital death and 14,451 were transferred to other facilities. The machine-learning-based model consisted of 11 predictors, showing a discrimination ability comparable to that using all the 26 variables (c-statistic: 0.760 [95% confidence interval, 0.752-0.767] vs. 0.761 [95% confidence interval, 0.753-0.769]). The common 1SE-selected variables identified throughout all analyses were low scores in activities of daily living, advanced age, absence of hypertension, impaired consciousness, failure to initiate enteral alimentation within 2 days and low body weight.
Conclusions: The developed machine learning model using 11 predictors had a good predictive ability to identify patients at high risk for non-home discharge. Our findings would contribute to the effective care coordination in this era when HF is rapidly increasing in prevalence.
Keywords: Claims database analysis; Clinical epidemiology; Heart failure; Machine learning; Non-home discharge.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Figures
Similar articles
-
Examination of independent predictors of discharge disposition in acute phase hospitalized heart failure patients undergoing phase I cardiac rehabilitation.Eur J Phys Rehabil Med. 2020 Dec;56(6):780-786. doi: 10.23736/S1973-9087.20.06347-9. Epub 2020 Oct 13. Eur J Phys Rehabil Med. 2020. PMID: 33047945
-
Early prediction of patient discharge disposition in acute neurological care using machine learning.BMC Health Serv Res. 2022 Oct 25;22(1):1281. doi: 10.1186/s12913-022-08615-w. BMC Health Serv Res. 2022. PMID: 36284297 Free PMC article.
-
Analysis of How Emergency Physicians' Decisions to Hospitalize or Discharge Patients With Acute Heart Failure Match the Clinical Risk Categories of the MEESSI-AHF Scale.Ann Emerg Med. 2019 Aug;74(2):204-215. doi: 10.1016/j.annemergmed.2019.03.010. Epub 2019 May 27. Ann Emerg Med. 2019. PMID: 31147102
-
A clinical score to predict mortality in patients after acute heart failure from Japanese registry.ESC Heart Fail. 2021 Dec;8(6):4800-4807. doi: 10.1002/ehf2.13664. Epub 2021 Oct 22. ESC Heart Fail. 2021. PMID: 34687170 Free PMC article.
-
Home Medications Contribute to a Unique Opportunity for Error on Discharge from the Hospital.2023 Jun 14. In: WebM&M: Case Studies [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Oct 30–. 2023 Jun 14. In: WebM&M: Case Studies [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Oct 30–. PMID: 40106631 Free Books & Documents. Review. No abstract available.
Cited by
-
Association Between Complementary Use of Daikenchuto (a Japanese Herbal Medicine) and Readmission in Older Patients With Heart Failure and Constipation.Circ Rep. 2025 Jan 21;7(2):86-96. doi: 10.1253/circrep.CR-24-0114. eCollection 2025 Feb 10. Circ Rep. 2025. PMID: 39931709 Free PMC article.
-
Performance of risk models to predict mortality risk for patients with heart failure: evaluation in an integrated health system.Clin Res Cardiol. 2024 Sep;113(9):1343-1354. doi: 10.1007/s00392-024-02433-2. Epub 2024 Apr 2. Clin Res Cardiol. 2024. PMID: 38565710
-
Children Comorbidity Score, a Simple Predictor for In-hospital Mortality: A Nationwide Inpatient Database Study in Japan.JMA J. 2025 Apr 28;8(2):568-579. doi: 10.31662/jmaj.2024-0333. Epub 2025 Apr 4. JMA J. 2025. PMID: 40415997 Free PMC article.
-
Machine learning in predicting heart failure survival: a review of current models and future prospects.Heart Fail Rev. 2025 Mar;30(2):431-442. doi: 10.1007/s10741-024-10474-y. Epub 2024 Dec 10. Heart Fail Rev. 2025. PMID: 39656330 Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
