

Feasibility of Reduced Clinical Monitoring in Patients with Inflammatory Bowel Disease Treated with Thiopurine Therapy
- PMID: 37131100
- PMCID: PMC10293334
- DOI: 10.1007/s10620-023-07950-0
Feasibility of Reduced Clinical Monitoring in Patients with Inflammatory Bowel Disease Treated with Thiopurine Therapy
Abstract
Background: Outpatient visits and laboratory assessments are routinely scheduled every 3 to 4 months in thiopurine-treated patients with inflammatory bowel disease (IBD) to timely detect thiopurine-related adverse events (AEs). AEs that require therapy adjustment beyond 12 months of treatment are rare.
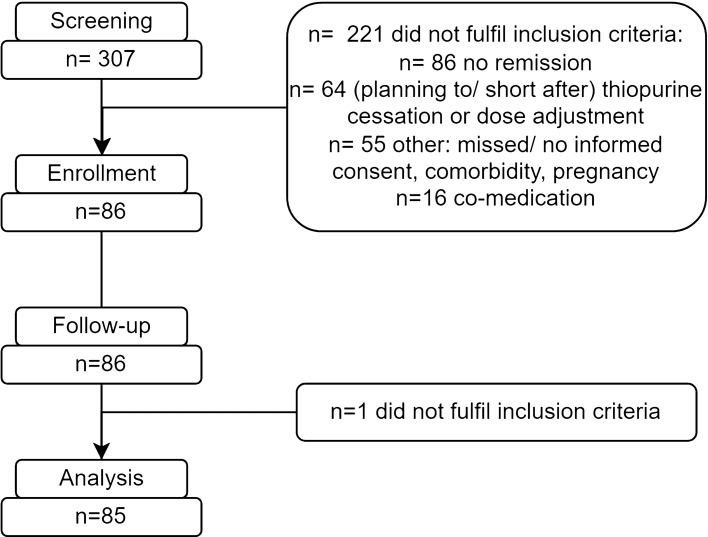
Aim and methods: This single-center prospective cohort study evaluated the safety of a reduced 6-monthly monitoring strategy in steroid-free patients with quiescent IBD on stable dose of azathioprine, mercaptopurine, or thioguanine monotherapy. The primary outcome was thiopurine-related AEs requiring therapy adjustments during a follow-up period of 24 months. Secondary outcomes included all AEs including laboratory toxicity, disease flares until 12 months, and the net monetary benefit from this strategy concerning IBD-related health care use.
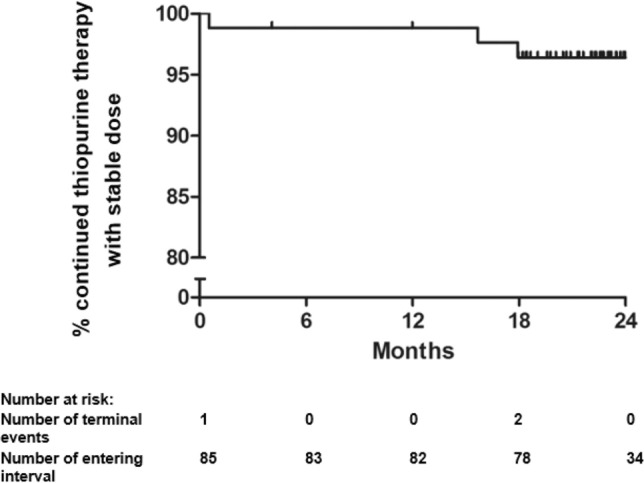
Results: We enrolled 85 patients with IBD (median age 42 years, 61% Crohn's disease, 62% female), with a median disease duration of 12.5 years and median thiopurine treatment duration of 6.7 years. During follow-up, 3 patients (4%) ceased thiopurines due to AEs: recurrent infections, non-melanoma skin cancer, and gastrointestinal complaints (nausea, vomiting). At 12 months, 25 laboratory toxicities were observed (including 13% myelotoxicity, 17% hepatotoxicity); none required therapy adjustments and all were transient. A reduced monitoring strategy had a net benefit of €136 per patient.
Conclusion: Three patients (4%) ceased thiopurine therapy due to thiopurine-related AEs, while no laboratory toxicity required therapy adjustments. Monitoring frequency of every 6 months seems feasible in patients with stable IBD on long-term (median duration > 6 years) maintenance thiopurine therapy and may contribute to reduced patient-burden and health care costs.
Keywords: Adverse events; Inflammatory bowel disease; Monitoring; Safety; Thiopurines.
© 2023. The Author(s).
Conflict of interest statement
D.J. de Jong received consulting fees from Synthon, Pharma, Abbvie, and MSD, and travel fees from Falk Pharma, Takeda, Abbvie, MSD, Ferring, Vifor Pharma, and Cablon Medical. F. Hoentjen has served on advisory boards, or as speaker or consultant for Abbvie, Celgene, Janssen-Cilag, MSD, Takeda, Teva, Sandoz, and Dr. Falk, and has received unrestricted grants from Dr. Falk, Janssen-Cilag, Abbvie, Takeda. Other authors have no potential conflict of interest to disclose.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
