

Depth of anesthesia, temperature, and postoperative delirium in children and adolescents undergoing cardiac surgery
- PMID: 37131120
- PMCID: PMC10152600
- DOI: 10.1186/s12871-023-02102-3
Depth of anesthesia, temperature, and postoperative delirium in children and adolescents undergoing cardiac surgery
Erratum in
-
Correction: Depth of anesthesia, temperature, and postoperative delirium in children and adolescents undergoing cardiac surgery.BMC Anesthesiol. 2023 Sep 15;23(1):312. doi: 10.1186/s12871-023-02272-0. BMC Anesthesiol. 2023. PMID: 37715153 Free PMC article. No abstract available.
Abstract
Background: After pediatric cardiosurgical interventions, postoperative delirium can occur, which can be associated with undesirable consequences during and after the hospital stay. It is therefore important to avoid any factors causing delirium as far as possible. Electroencephalogram (EEG) monitoring can be used during anesthesia to individually adjust dosages of hypnotically acting drugs. It is necessary to gain knowledge about the relationship between intraoperative EEG and postoperative delirium in children.
Methods: In a dataset comprising 89 children (53 male, 36 female; median age: 0.99 (interquartile range: 0.51, 4.89) years) undergoing cardiac surgery involving use of a heart-lung machine, relationships between depth of anesthesia as measured by EEG (EEG index: Narcotrend Index (NI)), sevoflurane dosage, and body temperature were analyzed. A Cornell Assessment of Pediatric Delirium (CAP-D) score ≥ 9 indicated delirium.
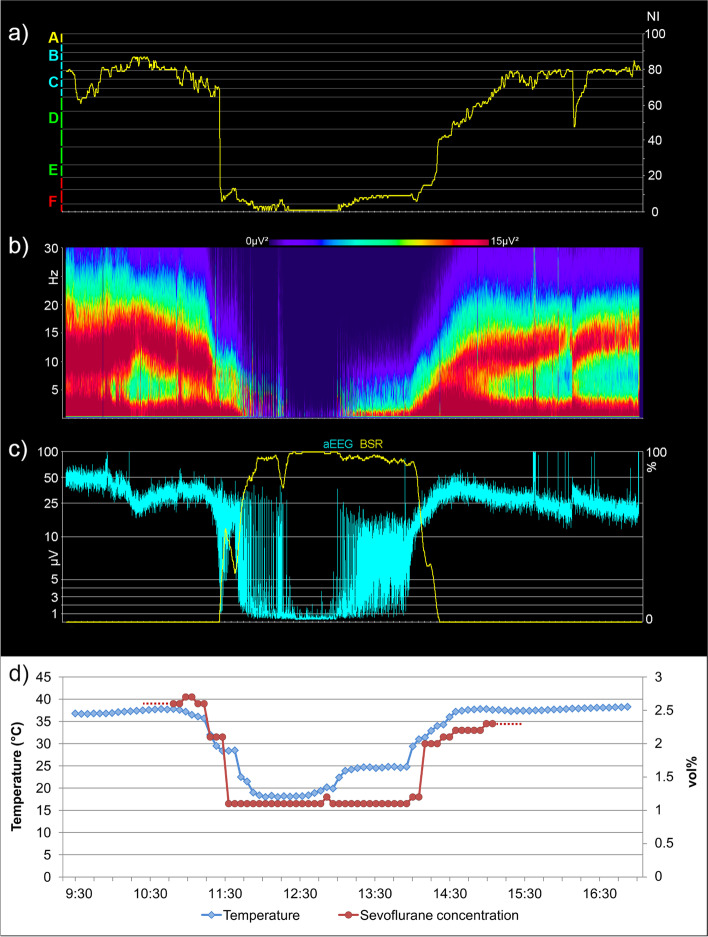
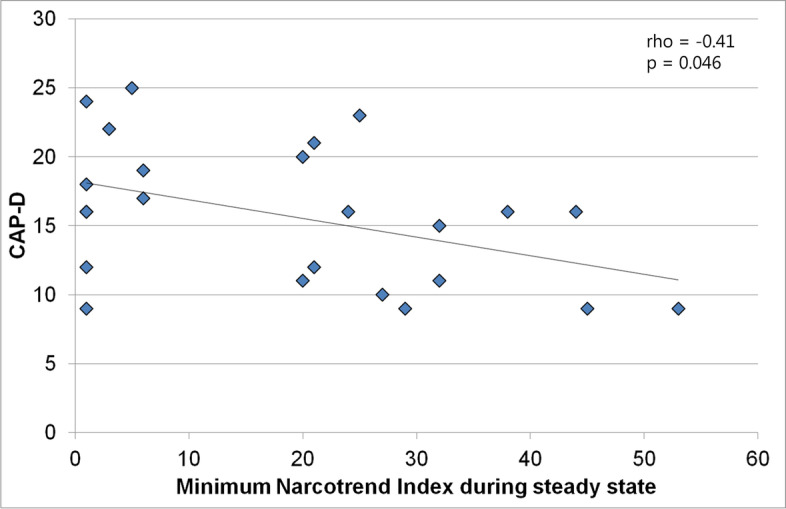
Results: The EEG could be used in patients of all age groups for patient monitoring during anesthesia. In the context of induced hypothermia, EEG monitoring supported individually adjusted sevoflurane dosing. The NI was significantly correlated with the body temperature; decreasing temperature was accompanied by a decreasing NI. A CAP-D score ≥ 9 was documented in 61 patients (68.5%); 28 patients (31.5%) had a CAP-D < 9. Delirious patients with an intubation time ≤ 24 h showed a moderate negative correlation between minimum NI (NImin) and CAP-D (rho = -0.41, 95% CI: -0.70 - -0.01, p = 0.046), i.e., CAP-D decreased with increasing NImin. In the analysis of all patients' data, NImin and CAP-D showed a weak negative correlation (rho = -0.21, 95% CI: -0.40 - 0.01, p = 0.064). On average, the youngest patients had the highest CAP-D scores (p = 0.002). Patients with burst suppression / suppression EEG had a longer median intubation time in the intensive care unit than patients without such EEG (p = 0.023). There was no relationship between minimum temperature and CAP-D score.
Conclusions: The EEG can be used to individually adjust sevoflurane dosing during hypothermia. Of the patients extubated within 24 h and classified as delirious, patients with deeper levels of anesthesia had more severe delirium symptoms than patients with lighter levels of anesthesia.
Keywords: Body temperature; Cardiac surgery; Delirium; Depth of anesthesia; EEG; Heart–lung machine.
© 2023. The Author(s).
Conflict of interest statement
HK, AD, ND, MSchm, and MSchu declare that they do not have competing interests. BS was involved in EEG evaluations of depth of anesthesia (Narcotrend); this does not affect the analysis described in this article.
Figures



References
-
- Lindinger A, Schwedler G, Hense HW. Prevalence of congenital heart defects in newborns in Germany: Results of the first registration year of the PAN Study (July 2006 to June 2007) Klin Padiatr. 2010;222:321–326. - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 5. Arlington, VA: American Psychiatric Association; 2013.
-
- Aldecoa C, Bettelli G, Bilotta F, Sanders RD, Audisio R, Borozdina A, et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34:192–214. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
