

Deployment of personnel to military operations: impact on mental health and social functioning
- PMID: 37131363
- PMCID: PMC8427986
- DOI: 10.4073/csr.2018.6
Deployment of personnel to military operations: impact on mental health and social functioning
Abstract
This Campbell systematic review examines the effects of deployment on mental health. The review summarizes evidence from 185 studies. All studies used observational data to quantify the effect of deployment. This review includes studies that evaluate the effects of deployment on mental health. A total of 185 studies were identified. However, only 40 of these were assessed to be of sufficient methodological quality to be included in the final analysis. The studies spanned the period from 1993 to 2017 and were mostly carried out in the USA, UK and Australia. The studies all had some important methodological weaknesses. None of the included studies used experimental designs (random assignment). Deployment to military operations negatively affects the mental health functioning of deployed military personnel. For assessments taken more than 24 months since exposure, we consistently found adverse effects of deployment on all mental health domains (PTSD, depression, substance abuse/dependence, and common mental disorders), particularly on PTSD. For assessments taken less than 24 months (or a variable number of months since exposure) the evidence was less consistent and in many instances inconclusive.
Plain language summary: Deployment to military operations negatively affects the mental health functioning of deployed military personnel: While additional research is needed, the current evidence strongly supports the notion that deployment negatively affects mental health functioning of deployed military personnel.What is this review about?: When military personnel are deployed to military operations abroad they face an increased risk of physical harm, and an increased risk of adverse shocks to their mental health.The primary condition under consideration is deployment to an international military operation. Deployment to a military operation is not a uniform condition; rather, it covers a range of scenarios. Military deployment is defined as performing military service in an operation at a location outside the home country for a limited time period, pursuant to orders.The review included studies that reported outcomes for individuals who had been deployed. This review looked at the effect of deployment on mental health outcomes. The mental health outcomes are: post-traumatic stress disorder (PTSD), major depressive disorder (MDD), common mental disorders (depression, anxiety and somatisation disorders) and substance-related disorders.By identifying the major effects of deployment on mental health and quantifying these effects, the review can inform policy development on deployment and military activity as well as post-deployment support for veterans. In this way the review enables decision-makers to prioritise key areas.What are the main findings of this review?: What studies are included?: This review includes studies that evaluate the effects of deployment on mental health. A total of 185 studies were identified. However, only 40 of these were assessed to be of sufficient methodological quality to be included in the final analysis. The studies spanned the period from 1993 to 2017 and were mostly carried out in the USA, UK and Australia. The studies all had some important methodological weaknesses. None of the included studies used experimental designs (random assignment).Does deployment have an effect on mental health?: Deployment to military operations negatively affects the mental health functioning of deployed military personnel. For assessments taken more than 24 months since exposure, we consistently found adverse effects of deployment on all mental health domains (PTSD, depression, substance abuse/dependence, and common mental disorders), particularly on PTSD. For assessments taken less than 24 months (or a variable number of months since exposure) the evidence was less consistent and in many instances inconclusive.What do the findings of this review mean?: The odds of screening positive for PTSD and depression were consistently high in the longer term. This suggests that efforts should be increased to detect and treat mental disorders, as effects may be long-lasting.Overall the risk of bias in the majority of included studies was high. While it is difficult to imagine a randomised study design to understand how deployment affects mental health, other matters such as changes to personnel policy, or unanticipated shocks to the demand for military personnel, could potentially be a rich source of quasi-experimental variation.How up-to-date is this review?: The review authors searched for studies up to 2017. This Campbell systematic review was published in March 2018.
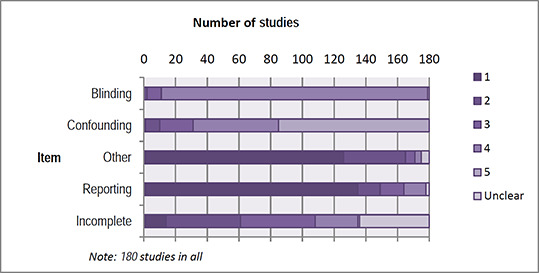
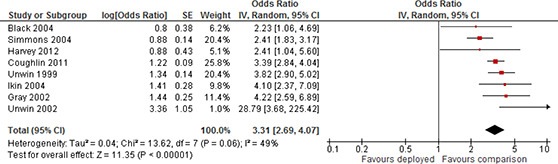
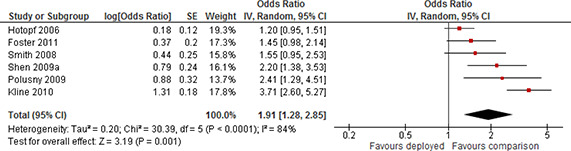
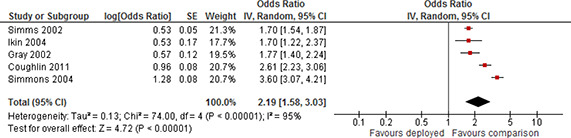
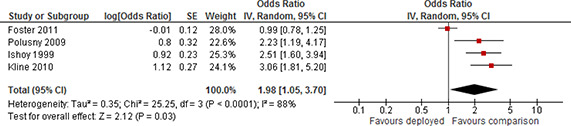
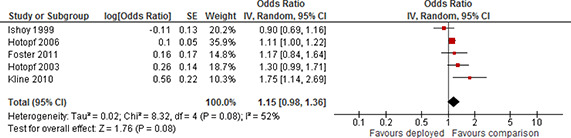
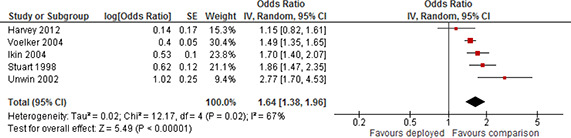
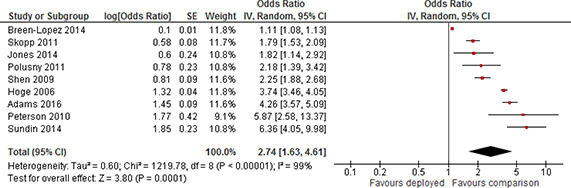
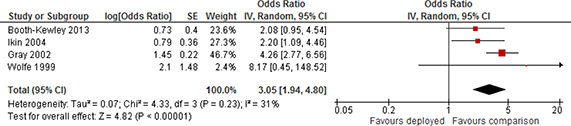
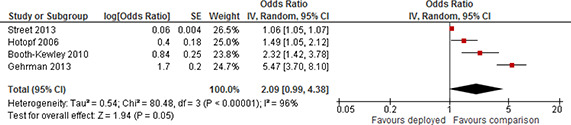
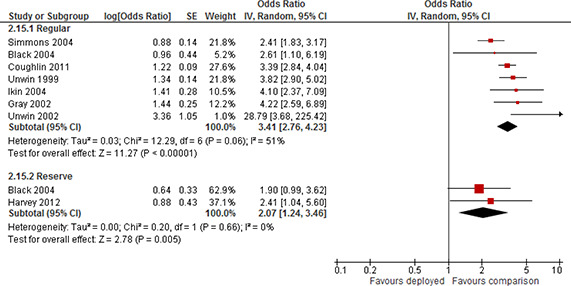
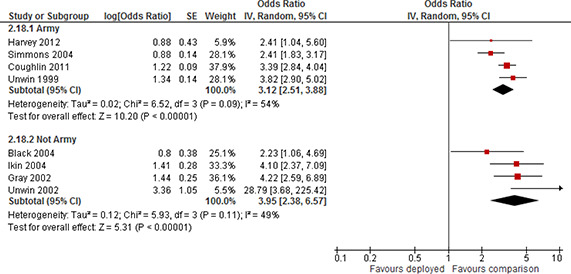
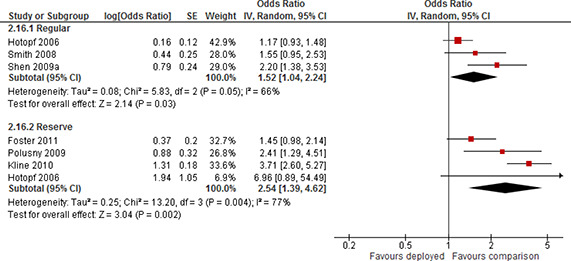
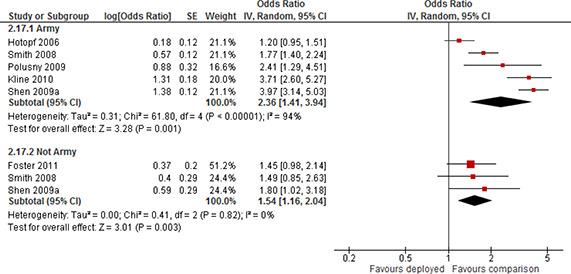
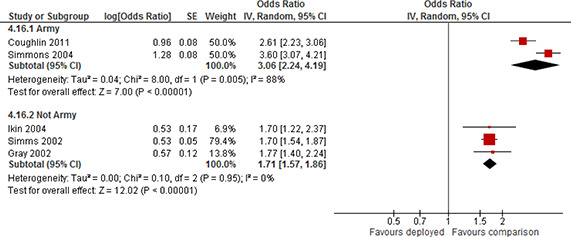
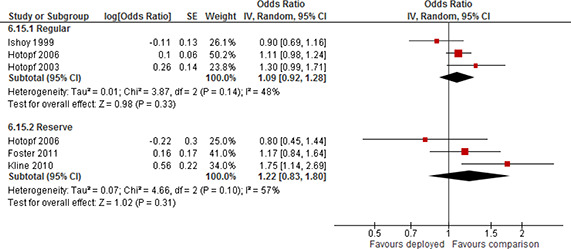
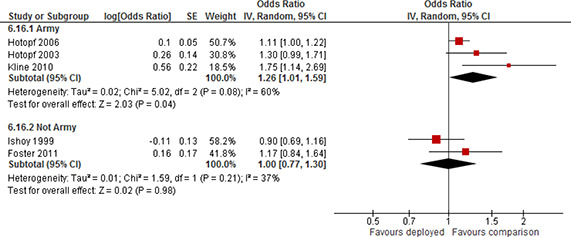
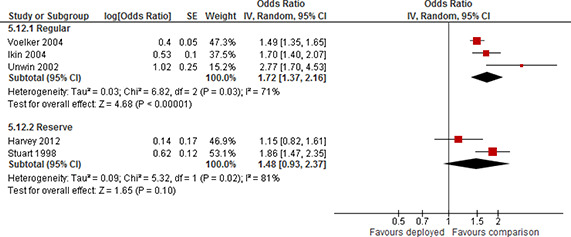
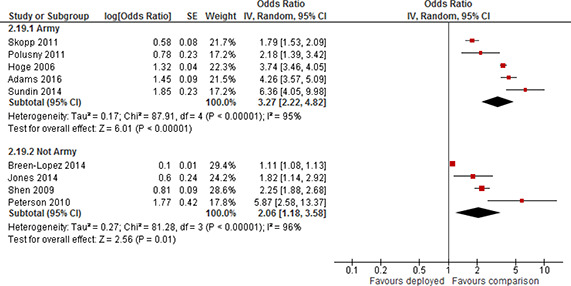
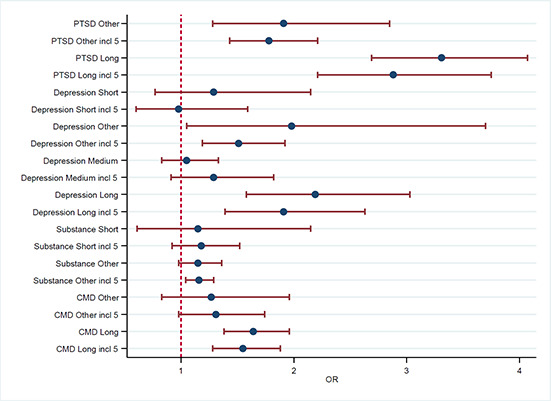
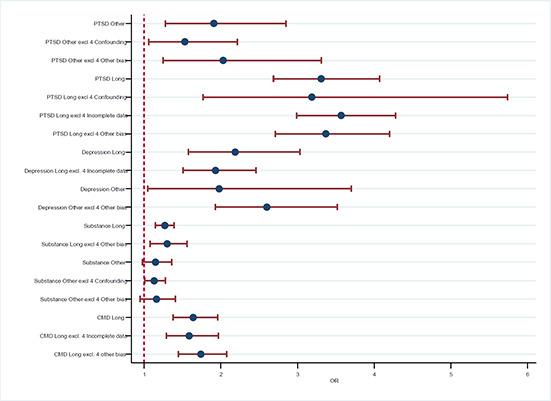
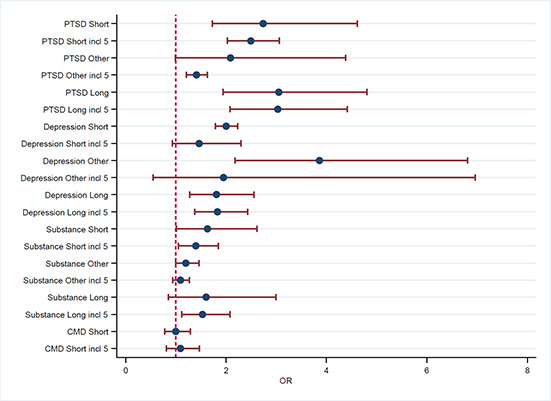
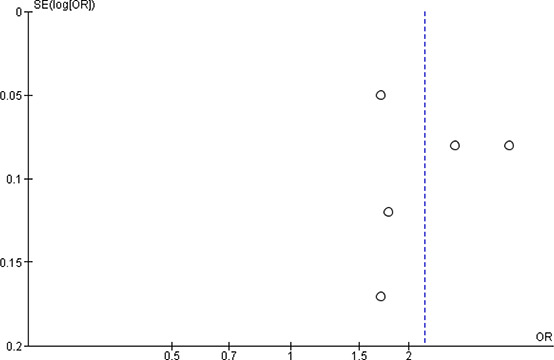
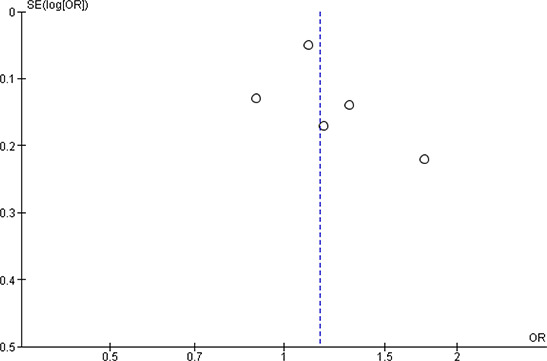
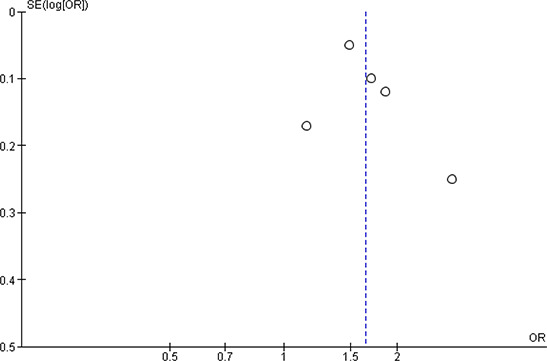
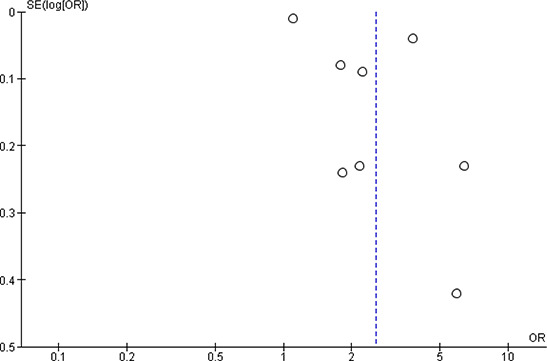
Executive summary: BACKGROUND: When military personnel are deployed to military operations abroad they face an increased risk of physical harm, and an increased risk of adverse shocks to their mental health. Research suggests that the increased risk to mental health is mainly due to the hazards of war, combat exposure: firing weapons, road side bombs, seeing fellow soldiers, friends, civilians, and enemies being injured, maimed or killed. These experiences may lead to severe mental stress. The adverse impact on mental health is the psychological cost of war, and it is of interest to policymakers to learn the magnitude of these effects. This review sets out to synthesise available evidence about the consequences of deployment for deployed military personnel in the mental health and social functioning domains.OBJECTIVES: The objective of this review isto synthesise the consequences of deployment to military operation on the mental health and social functioning of deployed military personnel.SEARCH METHODS: We searched electronic databases, grey literature, and references from primary studies and related reviews. No language or date restrictions were applied to the searches. We searched the following electronic databases: Academic Search Elite, Cochrane Library, EMBASE, ERIC, MEDLINE, PsycINFO, Science Citation Index, Social Science Citation Index, SocINDEX, as well as the Nordic platforms: bibliotek.dk, BIBSYS, and LIBRIS. The conclusions of this review are based on the most recent searches performed. The last search was performed in April 2017.SELECTION CRITERIA: Primary studies had to meet the following inclusion criteria: Participants: The participants should be military personnel.Intervention: The condition should be deployment to a military operation.Comparison: The relevant comparisons were either comparing a) deployed military personnel to non-deployed military personnel, b) deployed military personnel to military personnel deployed elsewhere, for example personnel deployed to non-combat operations, c) military personnel deployed to the same operation but stratified by combat exposure.Outcomes: The study should report on one or more mental health outcomes, and/or social functioning for the deployed participants. In particular studies should report on one or more of the following mental health outcomes: PTSD, major depression, substance abuse or dependence (including alcohol), and common mental disorders (depression and anxiety disorders). The following social functioning outcomes were relevant: employment, and homelessness.Study Designs: Both experimental and quasi-experimental designs with a comparison group were eligible for inclusion in the review. Studies were excluded if they: Reported on deployments taking place before 1989.Used a within group pre-post study design.Did not report on at least one of the mental health or social functioning outcomes. DATA COLLECTION AND ANALYSIS: The total number of potentially relevant studies constituted31,049records. A total of 185 studies met the inclusion criteria and were critically appraised by the review authors. The final selection of 185 studies was from 13 different countries.Forty eight of the 185 studies did not report effect estimates or provide data that would allow the calculation of an effect size and standard error. Fifty four studies were excluded because of overlapping samples. The majority of those studies were from USA but the main reason for not using studies from USA in the synthesis was lack of information to calculate an effect size. Nearly half the studies from the UK could not be used in the synthesis due to overlap of data samples. Forty three studies were judged to have a very high risk of bias (5 on the scale) and, in accordance with the protocol, we excluded these from the data synthesis on the basis that they would be more likely to mislead than inform., Thus a total of 40 studies, from five different countries, were included in the data synthesis.Random effects models were used to pool data across the studies. We used the odds ratio. Pooled estimates were weighted with inverse variance methods, and 95% confidence intervals were calculated. The meta-analyses were carried out by time since exposure (short, medium, long, and other time since exposure) and by type of comparison (deployed versus non-deployed, all deployed but stratified by either combat operations versus non-combat operations, or stratified by combat exposure). We performed single factor subgroup analysis. The assessment of any difference between subgroups was based on 95% confidence intervals. Funnel plots were used to assess the possibility of publication bias. Sensitivity analysis was used to evaluate whether the pooled effect sizes were robust across components of methodological quality.MAIN RESULTS: The findings were mixed, depending on the outcome, the time since exposure and the approach (deployed versus non-deployed termed absolute or stratified by extent of combat termed relative) used to investigate the effect. It was not possible to analyse the outcomes homelessness and employment. All studies that could be used in the data synthesis reported on the impact of deployment on mental health; PTSD, depression, substance use or common mental disorder.For assessments taken less than 24 months since exposure the evidence was inconclusive either because too few studies reported results in the short and medium term and/or the degree of heterogeneity between studies was large.For assessments taken at other time points (a variable number of months since exposure) the evidence was inconclusive for the relative comparisons due to either too few studies or a substantial degree of heterogeneity between studies. For the absolute comparison the analysis of common mental disorder was inconclusive, whereas the average effects of PTSD and depression were positive and statistically significant (PTSD odds ratio (OR) was 1.91 (95% confidence interval (CI): 1.28 to 2.85) and OR=1.98 (95% CI: 1.05 to 3.70) for depression). The analysis concerning substance use indicated that deployed participants did not have higher odds of screening positive for substance use compared to non-deployed participants (OR=1.15 (95% CI: 0.98 to 1.36)).For assessments taken more than 24 months post exposure, meta-analyses indicated that the odds of screening positive for PTSD, depression, substance use and common mental disorder were higher for participants in the deployed group compared to participants in the group that were not deployed (PTSD OR=3.31 (95% CI: 2.69 to 4.07), OR=2.19 (95% CI: 1.58 to 3.03) for depression, OR=1.27 (95% CI: 1.15 to 1.39) for substance use, and OR=1.64 (95% CI: 1.38 to 1.96) for common mental disorder). Likewise, participants reporting high combat exposure had higher odds of screening positive for PTSD and depression than participants reporting lower exposure for long term assessments (PTSD OR=3.05 (95% CI: 1.94 to 4.80) and OR=1.81 (95% CI: 1.28 to 2.56) for depression). The analyses of substance use and common mental disorder were inconclusive due to too few studies.On the basis of the prevalence of mental health problems in pre-deployed or non-deployed population based comparison sampleswe would therefore expect the long term prevalence of PTSD in post-deployed samples to be in the range 6.1 - 14.9%, the long term prevalence of depression to be in the range from 7.6% to 18%, the long term prevalence of substance use to be in the range from 2.4% to 17.5% and the prevalence of common mental disorder to be in the range from 10% to 23%.Sensitivity analyses resulted in no appreciable change in effect size, suggesting that the results are robust.It was only possible to assess the impact of two types of personnel characteristics (branch of service and duty/enlistment status) on the mental health outcomes. We found no evidence to suggest that the effect of deployment on any outcomes differ between these two types of personnel characteristics.AUTHORS' CONCLUSIONS: Deployment to military operations negatively affects the mental health functioning of deployed military personnel. We focused on the effect of deployment on PTSD (post-traumatic stress disorder), depression, substance abuse/dependence, and common mental disorders (depression and anxiety disorders). For assessments taken less than 24 months (or a variable number of months since exposure) the evidence was less consistent and in many instances inconclusive. For assessments taken more than 24 months since exposure, we consistently found adverse effects of deployment on all domains, particularly on PTSD. There is increased political awareness of the need to address post deployment mental health problems. The odds of screening positive for PTSD and depression were consistently high in the longer term. This suggests that efforts should be increased to detect and treat mental disorders, as effects may be long lasting. Mental illness is of particular concern in the military for operational reasons, but they may be hard to detect in the military setting because a military career is intimately linked with mental and physical strength.It was not possible to examine a number of factors which we had reason to expect would impact on the magnitude of the effect. This would have been particularly relevant from a policy perspective because these are direct parameters that one could use to optimally "organize" deployment in order to minimize impacts on mental health functioning.While additional research is needed, the current evidence strongly supports the notion that deployment negatively affects mental health functioning of deployed military personnel. The next step is to begin to examine preventive measures and policies for organizing deployment, in order to minimize the effects on mental health.
© 2018 Bøg et al.
Figures














Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Small class sizes for improving student achievement in primary and secondary schools: a systematic review.Campbell Syst Rev. 2018 Oct 11;14(1):1-107. doi: 10.4073/csr.2018.10. eCollection 2018. Campbell Syst Rev. 2018. PMID: 37131395 Free PMC article.
-
Recovery schools for improving behavioral and academic outcomes among students in recovery from substance use disorders: a systematic review.Campbell Syst Rev. 2018 Oct 4;14(1):1-86. doi: 10.4073/csr.2018.9. eCollection 2018. Campbell Syst Rev. 2018. PMID: 37131375 Free PMC article.
-
Voluntary work for the physical and mental health of older volunteers: A systematic review.Campbell Syst Rev. 2020 Oct 23;16(4):e1124. doi: 10.1002/cl2.1124. eCollection 2020 Dec. Campbell Syst Rev. 2020. PMID: 37016617 Free PMC article. Review.
-
Reducing unemployment benefit duration to increase job finding rates: a systematic review.Campbell Syst Rev. 2018 Feb 28;14(1):1-194. doi: 10.4073/csr.2018.2. eCollection 2018. Campbell Syst Rev. 2018. PMID: 37131392 Free PMC article.
Cited by
-
Do children separated from fathers have higher anxiety levels? A comparative analysis.Med J Armed Forces India. 2023 May-Jun;79(3):316-320. doi: 10.1016/j.mjafi.2021.06.005. Epub 2021 Aug 13. Med J Armed Forces India. 2023. PMID: 37193532 Free PMC article.
-
STRONG STAR and the Consortium to Alleviate PTSD: Shaping the future of combat PTSD and related conditions in military and veteran populations.Contemp Clin Trials. 2021 Nov;110:106583. doi: 10.1016/j.cct.2021.106583. Epub 2021 Sep 29. Contemp Clin Trials. 2021. PMID: 34600107 Free PMC article.
-
Cumulative incidence of mental disorders in military personnel after 20 years of war in Afghanistan and 10 years in Mali - a comparison.Eur J Psychotraumatol. 2025 Dec;16(1):2477422. doi: 10.1080/20008066.2025.2477422. Epub 2025 Mar 17. Eur J Psychotraumatol. 2025. PMID: 40094959 Free PMC article.
-
Impact of life-threatening military incidents during deployments abroad on the relationships between military personnel and their families.Front Psychiatry. 2024 Jul 18;15:1419022. doi: 10.3389/fpsyt.2024.1419022. eCollection 2024. Front Psychiatry. 2024. PMID: 39091456 Free PMC article.
References
7 References
7.1 REFERENCES TO INCLUDED STUDIES
-
- Adler, A. B., Britt, T. W., Castro, C. A., McGurk, D., & Bliese, P. D. (2011). Effect of transition home from combat on risk‐taking and health‐related behaviors. Journal of Traumatic Stress, 24, 381–389. - PubMed
-
- Afari, N., Pittman, J., Floto, E., Owen, L., Buttner, M., Hossain, N., … & Lohr, J. B. (2015). Differential impact of combat on postdeployment symptoms in female and male veterans of Iraq and Afghanistan. Military Medicine, 180(3), 296–303. - PubMed
-
- Al‐Turkait, F. A. & Ohaeri, J. U. (2008). Prevalence and correlates of posttraumatic stress disorder among Kuwaiti military men according to level of involvement in the first Gulf War. Depression & Anxiety, 25, 932–941. - PubMed
-
- Axelrod, S. R., Morgan, C. A., III, & Southwick, S. M. (2005). Symptoms of posttraumatic stress disorder and borderline personality disorder in veterans of Operation Desert Storm. American Journal of Psychiatry, 162, 270–275. - PubMed
7.2 REFERENCES TO EXCLUDED STUDIES [REASON]
-
- Bell, N. S., Amoroso, P. J., Williams, J. O., Yore, M. M., Engel, J., Senier, L. et al. (2010). Demographic, Physical, and Mental Health Factors Associated With Deployment of U.S. Army Soldiers to the Persian Gulf. Military Medicine, 175, 227–237. [Selection into deployment] - PubMed
-
- Engelhard, I. M., van, D. H. , Marcel, A., & Lommen Miriam, J. J. (2009). Individuals high in neuroticism are not more reactive to adverse events. Personality and Individual Differences, 47, 697–700. [No relevant outcome]
-
- Forbes, D., Fletcher, S., Phelps, A., Wade, D., Creamer, M., & O'Donnell, M. (2013). Impact of combat and non‐military trauma exposure on symptom reduction following treatment for veterans with posttraumatic stress disorder. Psychiatry Research, 206, 33–36. [Veterans in treatment for PTSD and how CE is linked to severity of PTSD] - PubMed
-
- Forman‐Hoffman, V. L., Peloso, P. M., Black, D. W., Woolson, R. F., Letuchy, E. M., & Doebbeling, B. N. (2007). Chronic widespread pain in veterans of the first Gulf War: Impact of deployment status and associated health effects. The Journal of Pain, 8, 954–961.[No relevant outcome] - PubMed
7.3 ADDITIONAL REFERENCES
-
- American Psychiatric Association . (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC.
-
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC.
-
- Andersen, H.E. (1998). Danske FN‐soldater ‐ 2 år efter: Opfølgningsundersøgelse af DANBAT 7 & 8. [Danish UN soldiers ‐ 2 years after: follow‐up study of DANBAT 7 & 8]. FCL Publikation 144.
-
- Angrist, J. D., Chen, S. H., & Frandsen, B. R. (2010). Did Vietnam veterans get sicker in the 1990s? The complicated effects of military service on self‐reported health. Journal of Public Economics, 94(11), 824–837.
-
- Atkinson, M.P., Guetz A., & Wein L.M. (2009): A Dynamic Model for Posttraumatic Stress Disorder Among U.S. Troops in Operation Iraqi Freedom. Management Science, 55(9), 1454–1468.
LinkOut - more resources
Full Text Sources
Miscellaneous