

This is a preprint.
E-WE thrombin, a protein C activator, reduces disease severity and spinal cord inflammation in relapsing-remitting murine experimental autoimmune encephalomyelitis
- PMID: 37131631
- PMCID: PMC10153372
- DOI: 10.21203/rs.3.rs-2802415/v1
E-WE thrombin, a protein C activator, reduces disease severity and spinal cord inflammation in relapsing-remitting murine experimental autoimmune encephalomyelitis
Abstract
Objective: Relapses in patients with relapsing-remitting multiple sclerosis (RRMS) are typically treated with high-dose corticosteroids including methylprednisolone. However, high-dose corticosteroids are associated with significant adverse effects, can increase the risk for other morbidities, and often do not impact disease course. Multiple mechanisms are proposed to contribute to acute relapses in RRMS patients, including neuroinflammation, fibrin formation and compromised blood vessel barrier function. The protein C activator, E-WE thrombin is a recombinant therapeutic in clinical development for its antithrombotic and cytoprotective properties, including protection of endothelial cell barrier function. In mice, treatment with E-WE thrombin reduced neuroinflammation and extracellular fibrin formation in myelin oligodendrocyte glycoprotein (MOG)-induced experimental autoimmune encephalomyelitis (EAE). We therefore tested the hypothesis that E-WE thrombin could reduce disease severity in a relapsing-remitting model of EAE.
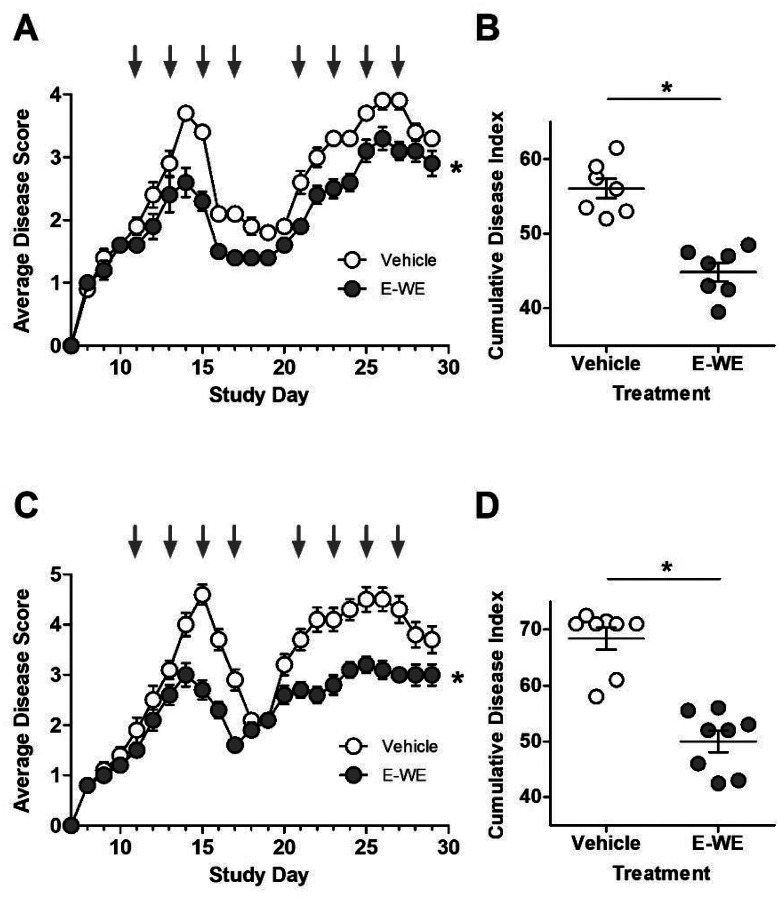
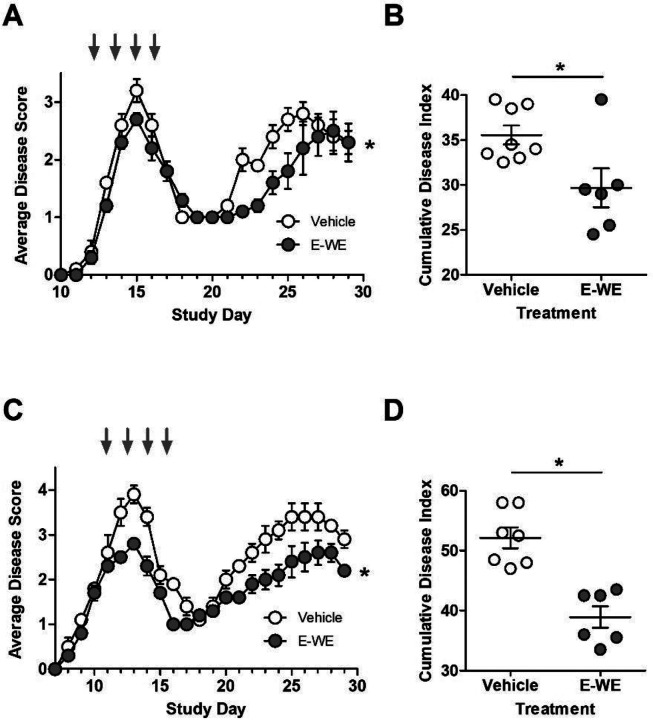
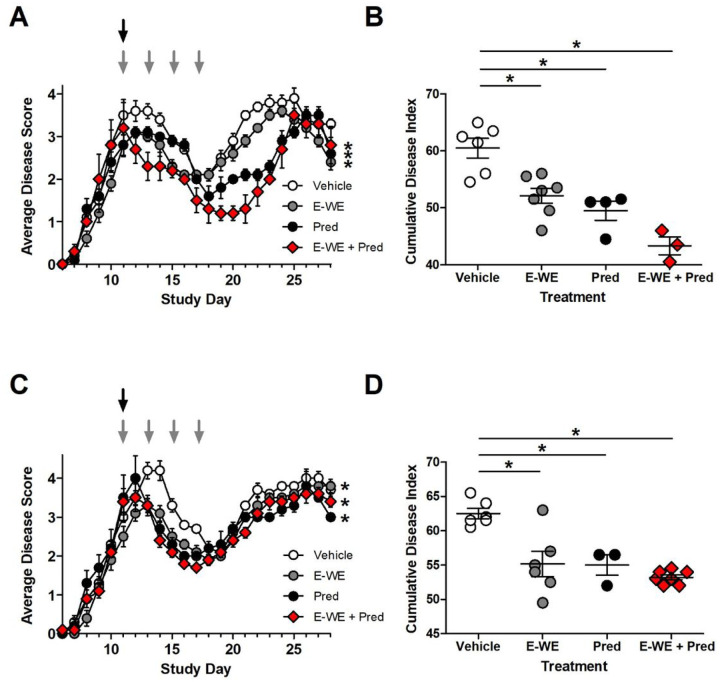
Methods: Female SJL mice were inoculated with proteolipid protein (PLP) peptide and treated with E-WE thrombin (25 μg/kg; iv) or vehicle at onset of detectable disease. In other experiments, E-WE thrombin was compared to methylprednisolone (100 mg/kg; iv) or the combination of both.
Results: Compared to vehicle, administration of E-WE thrombin significantly improved disease severity of the initial attack and relapse and delayed onset of relapse as effectively as methylprednisolone. Both methylprednisolone and E-WE thrombin reduced demyelination and immune cell recruitment, and the combination of both treatments had an additive effect.
Conclusion: The data presented herein demonstrate that E-WE thrombin is protective in mice with relapsing-remitting EAE, a widely used model of MS. Our data indicate that E-WE thrombin is as effective as high-dose methylprednisolone in improving disease score and may exert additional benefit when administered in combination. Taken together, these data suggest that E-WE thrombin may be an effective alternative to high-dose methylprednisolone for managing acute MS attacks.
Keywords: Animal model; Demyelination; Inflammation; Multiple sclerosis; Relapsing/remitting; Steroids; Thrombin.
Conflict of interest statement
Competing Interests NV and ET are employees of Aronora, Inc. and Oregon Health Science University (OHSU). This potential conflict of interest has been reviewed and managed by the OHSU Conflict of Interest in Research Committee. The remaining authors declare no competing financial interests.
Figures


References
-
- Cossburn M., et al. Autoimmune disease after alemtuzumab treatment for multiple sclerosis in a multicenter cohort. Neurology 77, 573–579 (2011). - PubMed
-
- Oliveri R.L., et al. Randomized trial comparing two different high doses of methylprednisolone in MS: a clinical and MRI study. Neurology 50, 1833–1836 (1998). - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
