

The learning curves of major laparoscopic and robotic procedures in urology: a systematic review
- PMID: 37132184
- PMCID: PMC10389344
- DOI: 10.1097/JS9.0000000000000345
The learning curves of major laparoscopic and robotic procedures in urology: a systematic review
Abstract
Background: Urology has been at the forefront of adopting laparoscopic and robot-assisted techniques to improve patient outcomes. This systematic review aimed to examine the literature relating to the learning curves of major urological robotic and laparoscopic procedures.
Methods: In accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a systematic literature search strategy was employed across PubMed, EMBASE, and the Cochrane Library from inception to December 2021, alongside a search of the grey literature. Two independent reviewers completed the article screening and data extraction stages using the Newcastle-Ottawa Scale as a quality assessment tool. The review was reported in accordance with AMSTAR (A MeaSurement Tool to Assess systematic Reviews) guidelines.
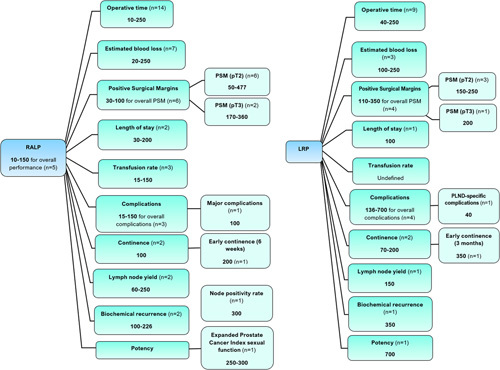
Results: Of 3702 records identified, 97 eligible studies were included for narrative synthesis. Learning curves are mapped using an array of measurements including operative time (OT), estimated blood loss, complication rates as well as procedure-specific outcomes, with OT being the most commonly used metric by eligible studies. The learning curve for OT was identified as 10-250 cases for robot-assisted laparoscopic prostatectomy and 40-250 for laparoscopic radical prostatectomy. The robot-assisted partial nephrectomy learning curve for warm ischaemia time is 4-150 cases. No high-quality studies evaluating the learning curve for laparoscopic radical cystectomy and for robotic and laparoscopic retroperitoneal lymph node dissection were identified.
Conclusion: There was considerable variation in the definitions of outcome measures and performance thresholds, with poor reporting of potential confounders. Future studies should use multiple surgeons and large sample sizes of cases to identify the currently undefined learning curves for robotic and laparoscopic urological procedures.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Baldev Chahal, Abdullatif Aydin, Mohammad S.A. Amin, Azhar Khan, Muhammad S. Khan and Kamran Ahmed have no conflicts of interest or financial ties to disclose. Prokar Dasgupta declares financial ties as Chief Medical Officer for Proximie Ltd. and Chief Scientific Officer for MysteryVibe Ltd. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures



References
-
- Wright TP. Factors affecting the cost of airplanes. J Aeronaut Sci 1936;3:122–128.
-
- Eden CG, Arora A, Hutton A. Cancer control, continence, and potency after laparoscopic radical prostatectomy beyond the learning and discovery curves. J Endourol 2011;25:815–819. - PubMed
-
- Satava RM, Gallagher AG, Pellegrini CA. Surgical competence and surgical proficiency: definitions, taxonomy, and metrics. J Am Coll Surg 2003;196:933–937. - PubMed
-
- Khan N, Abboudi H, Khan MS, et al. . Measuring the surgical ‘learning curve’: methods, variables and competency. BJU Int 2013;113:504–508. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
