

Outcomes following oropharyngeal squamous cell carcinoma resection and bilateral neck dissection with or without contralateral postoperative radiotherapy of the pathologically node-negative neck
- PMID: 37133497
- PMCID: PMC10313843
- DOI: 10.1007/s00405-023-07972-4
Outcomes following oropharyngeal squamous cell carcinoma resection and bilateral neck dissection with or without contralateral postoperative radiotherapy of the pathologically node-negative neck
Abstract
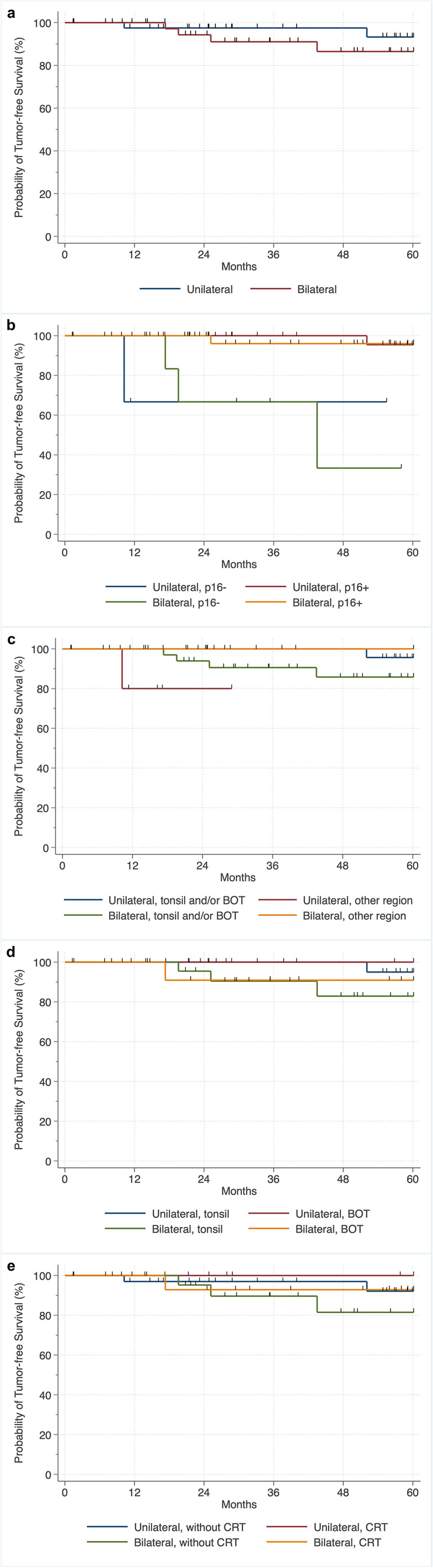
Purpose: There are no consensus guidelines regarding the postoperative treatment of the contralateral pathologically node-negative neck in oropharyngeal squamous cell carcinoma. This study aimed to determine if omission of postoperative irradiation of the contralateral pathologically node-negative neck affects oncological outcomes.
Methods: We retrospectively identified 84 patients with primary surgical treatment including bilateral neck dissection and postoperative (chemo-)radiotherapy (PO(C)RT). Survival was analyzed using the log-rank test and the Kaplan-Meier method.
Results: Patients showed no decrease in tumor-free, cause-specific (CSS), or overall survival (OS) when PO(C)RT of the contralateral pathologically node-negative neck was omitted. Increased OS was found in patients with unilateral PO(C)RT and especially an increased OS and CSS was found in unilateral PO(C)RT and in tumors arising from lymphoepithelial tissue.
Conclusions: Omitting the contralateral pathologically node-negative neck appears to be safe in terms of survival and our retrospective study advocates further prospective randomized control de-escalation trials.
Keywords: Adjuvant treatment; Contralateral neck; HPV; Neck irradiation; Oropharyngeal cancer.
© 2023. The Author(s).
Conflict of interest statement
The authors have no financial or non-financial interests to disclose.
Figures


Similar articles
-
Patterns of cervical node positivity, regional failure rates, and fistula rates for HPV+ oropharyngeal squamous cell carcinoma treated with transoral robotic surgery (TORS).Oral Oncol. 2018 Nov;86:296-300. doi: 10.1016/j.oraloncology.2018.10.001. Epub 2018 Oct 13. Oral Oncol. 2018. PMID: 30409315
-
Primary transoral robotic surgery with concurrent neck dissection for early stage oropharyngeal squamous cell carcinoma implemented at a Danish head and neck cancer center: a phase II trial on feasibility and tumour margin status.Eur Arch Otorhinolaryngol. 2017 May;274(5):2229-2237. doi: 10.1007/s00405-016-4433-3. Epub 2017 Jan 3. Eur Arch Otorhinolaryngol. 2017. PMID: 28050651 Clinical Trial.
-
Lymph node metastasis in level IIb in oropharyngeal squamous cell carcinoma: a multicentric, longitudinal, retrospective analysis.Eur Arch Otorhinolaryngol. 2023 Feb;280(2):869-876. doi: 10.1007/s00405-022-07647-6. Epub 2022 Sep 14. Eur Arch Otorhinolaryngol. 2023. PMID: 36102986
-
Occult lymph node metastasis in the contralateral neck of oropharyngeal squamous cell carcinoma: a meta-analysis and literature review.Eur Arch Otorhinolaryngol. 2022 Apr;279(4):2157-2166. doi: 10.1007/s00405-021-07230-5. Epub 2022 Jan 18. Eur Arch Otorhinolaryngol. 2022. PMID: 35041065 Review.
-
Management of oropharyngeal squamous cell carcinoma.Cancer Radiother. 2022 Feb-Apr;26(1-2):174-188. doi: 10.1016/j.canrad.2021.10.002. Epub 2021 Dec 22. Cancer Radiother. 2022. PMID: 34953693 Review.
Cited by
-
The Oncologic Outcomes of Bilateral Central Lymph Node Dissection in Unilobar Papillary Thyroid Cancer and Its Risks: A Prospective Cohort Study.Cureus. 2024 Jul 26;16(7):e65443. doi: 10.7759/cureus.65443. eCollection 2024 Jul. Cureus. 2024. PMID: 39184776 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
