

Computed high-b-value high-resolution DWI improves solid lesion detection in IPMN of the pancreas
- PMID: 37133518
- PMCID: PMC10511579
- DOI: 10.1007/s00330-023-09661-6
Computed high-b-value high-resolution DWI improves solid lesion detection in IPMN of the pancreas
Abstract
Objectives: To examine the effect of high-b-value computed diffusion-weighted imaging (cDWI) on solid lesion detection and classification in pancreatic intraductal papillary mucinous neoplasm (IPMN), using endoscopic ultrasound (EUS) and histopathology as a standard of reference.
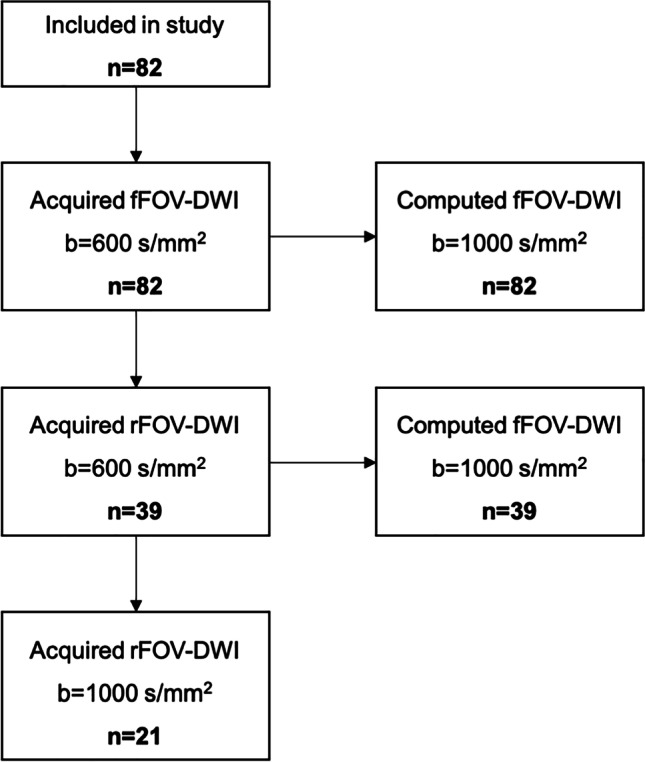
Methods: Eighty-two patients with known or suspected IPMN were retrospectively enrolled. Computed high-b-value images at b = 1000 s/mm2 were calculated from standard (b = 0, 50, 300, and 600 s/mm2) DWI images for conventional full field-of-view (fFOV, 3 × 3 × 4 mm3 voxel size) DWI. A subset of 39 patients received additional high-resolution reduced-field-of-view (rFOV, 2.5 × 2.5 × 3 mm3 voxel size) DWI. In this cohort, rFOV cDWI was compared against fFOV cDWI additionally. Two experienced radiologists evaluated (Likert scale 1-4) image quality (overall image quality, lesion detection and delineation, fluid suppression within the lesion). In addition, quantitative image parameters (apparent signal-to-noise ratio (aSNR), apparent contrast-to-noise ratio (aCNR), contrast ratio (CR)) were assessed. Diagnostic confidence regarding the presence/absence of diffusion-restricted solid nodules was assessed in an additional reader study.
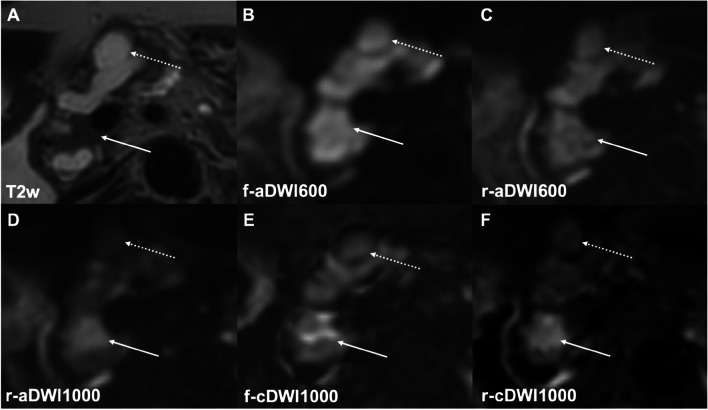
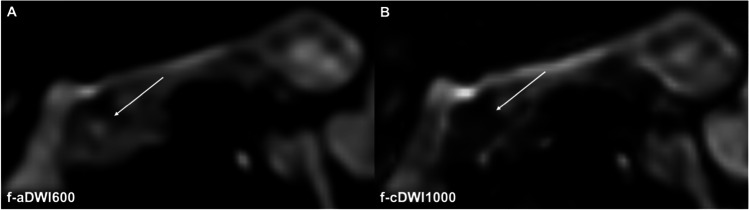
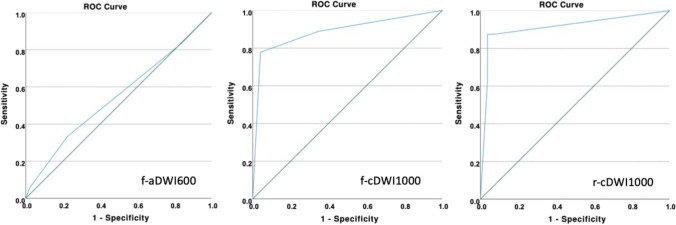
Results: High-b-value cDWI at b = 1000 s/mm2 outperformed acquired DWI at b = 600 s/mm2 regarding lesion detection, fluid suppression, aCNR, CR, and lesion classification (p = < .001-.002). Comparing cDWI from fFOV and rFOV revealed higher image quality in high-resolution rFOV-DWI compared to conventional fFOV-DWI (p ≤ .001-.018). High-b-value cDWI images were rated non-inferior to directly acquired high-b-value DWI images (p = .095-.655).
Conclusions: High-b-value cDWI may improve the detection and classification of solid lesions in IPMN. Combining high-resolution imaging and high-b-value cDWI may further increase diagnostic precision.
Clinical relevance statement: This study shows the potential of computed high-resolution high-sensitivity diffusion-weighted magnetic resonance imaging for solid lesion detection in pancreatic intraductal papillary mucinous neoplasia (IPMN). The technique may enable early cancer detection in patients under surveillance.
Key points: • Computed high-b-value diffusion-weighted imaging (cDWI) may improve the detection and classification of intraductal papillary mucinous neoplasms (IPMN) of the pancreas. • cDWI calculated from high-resolution imaging increases diagnostic precision compared to cDWI calculated from conventional-resolution imaging. • cDWI has the potential to strengthen the role of MRI for screening and surveillance of IPMN, particularly in view of the rising incidence of IPMNs combined with now more conservative therapeutic approaches.
Keywords: Diffusion magnetic resonance imaging, Pancreas; Pancreatic neoplasms, Pancreatic cysts.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
Kilian Weiss is an employee of Philips Healthcare.
Figures


References
-
- Adsay V, Mino-Kenudson M, Furukawa T, et al. Pathologic evaluation and reporting of intraductal papillary mucinous neoplasms of the pancreas and other tumoral intraepithelial neoplasms of pancreatobiliary tract: recommendations of Verona Consensus Meeting. Ann Surg. 2016;263:162–177. doi: 10.1097/SLA.0000000000001173. - DOI - PMC - PubMed
-
- Vege SS, Ziring B, Jain R, Moayyedi P (2015) American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 148:819–822 quize812-813 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
