

Reappraisal of Idiopathic CD4 Lymphocytopenia at 30 Years
- PMID: 37133586
- PMCID: PMC10239023
- DOI: 10.1056/NEJMoa2202348
Reappraisal of Idiopathic CD4 Lymphocytopenia at 30 Years
Abstract
Background: Idiopathic CD4 lymphocytopenia (ICL) is a clinical syndrome that is defined by CD4 lymphopenia of less than 300 cells per cubic millimeter in the absence of any primary or acquired cause of immunodeficiency. Some 30 years after its original identification, ICL has remained a disease of obscure cause, with limited evidence with respect to its prognosis or management, despite diagnostic and therapeutic innovations.
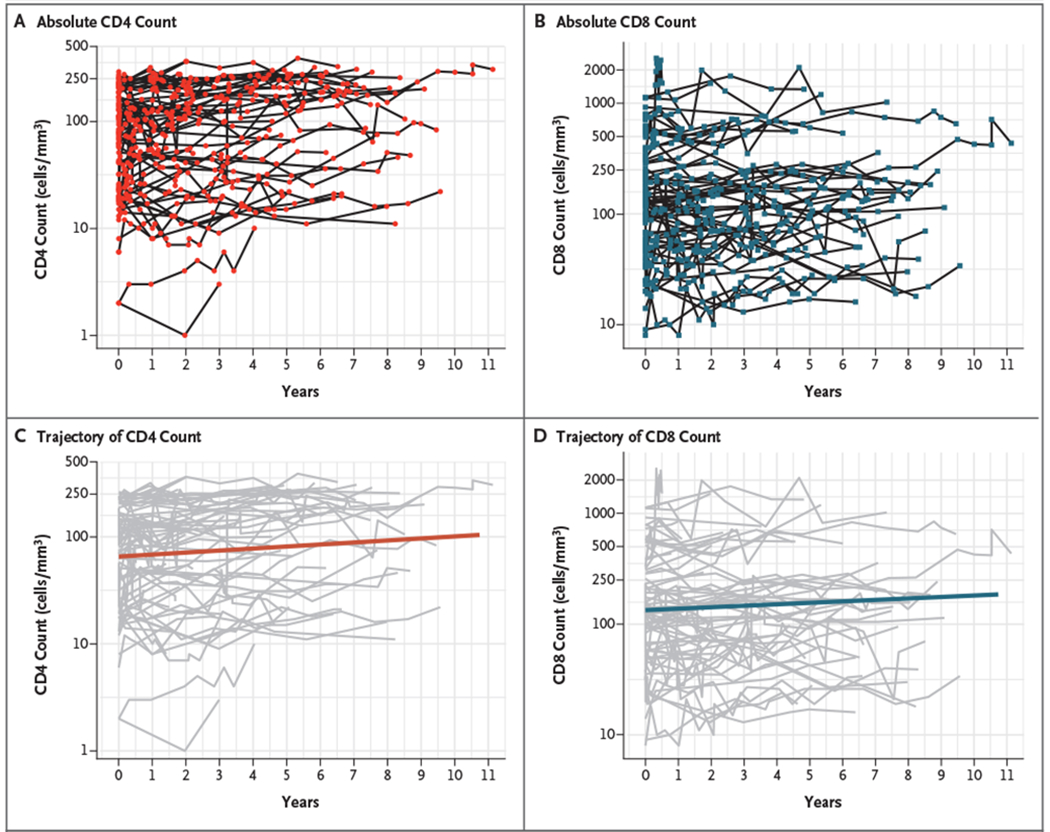
Methods: We evaluated the clinical, genetic, immunologic, and prognostic characteristics of 108 patients who were enrolled during an 11-year period. We performed whole-exome and targeted gene sequencing to identify genetic causes of lymphopenia. We also performed longitudinal linear mixed-model analyses of T-cell count trajectories and evaluated predictors of clinical events, the response to immunization against coronavirus disease 2019 (Covid-19), and mortality.
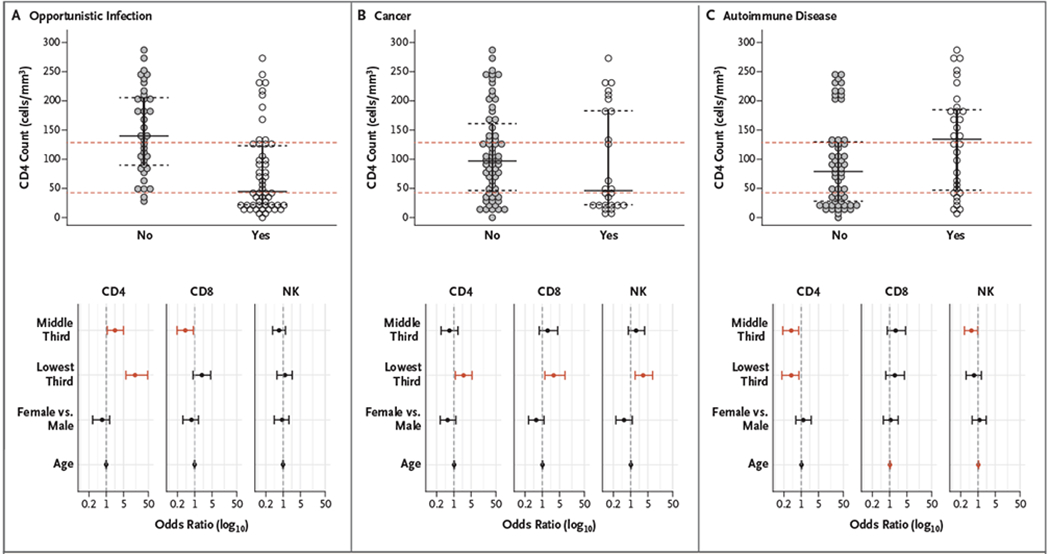
Results: After the exclusion of patients with genetic and acquired causes of CD4 lymphopenia, the study population included 91 patients with ICL during 374 person-years of follow-up. The median CD4+ T-cell count among the patients was 80 cells per cubic millimeter. The most prevalent opportunistic infections were diseases related to human papillomavirus (in 29%), cryptococcosis (in 24%), molluscum contagiosum (in 9%), and nontuberculous mycobacterial diseases (in 5%). A reduced CD4 count (<100 cells per cubic millimeter), as compared with a CD4 count of 101 to 300 cells, was associated with a higher risk of opportunistic infection (odds ratio, 5.3; 95% confidence interval [CI], 2.8 to 10.7) and invasive cancer (odds ratio, 2.1; 95% CI, 1.1 to 4.3) and a lower risk of autoimmunity (odds ratio, 0.5; 95% CI, 0.2 to 0.9). The risk of death was similar to that in the age- and sex-adjusted general population, but the prevalence of cancer was higher.
Conclusions: Among the study patients, ICL continued to be associated with increased susceptibility to viral, encapsulated fungal, and mycobacterial diseases, as well as with a reduced response to novel antigens and an increased risk of cancer. (Funded by the National Institute of Allergy and Infectious Diseases and the National Cancer Institute; ClinicalTrials.gov number, NCT00867269.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Idiopathic CD4 Lymphocytopenia at 30 Years.N Engl J Med. 2023 Aug 17;389(7):674. doi: 10.1056/NEJMc2307362. N Engl J Med. 2023. PMID: 37585645 No abstract available.
-
Idiopathic CD4 Lymphocytopenia at 30 Years.N Engl J Med. 2023 Aug 17;389(7):674-675. doi: 10.1056/NEJMc2307362. N Engl J Med. 2023. PMID: 37585646 No abstract available.
-
Idiopathic CD4 Lymphocytopenia at 30 Years. Reply.N Engl J Med. 2023 Aug 17;389(7):675-676. doi: 10.1056/NEJMc2307362. N Engl J Med. 2023. PMID: 37585647 No abstract available.
References
-
- Centers for Disease Control. Unexplained CD4+ T-lymphocyte depletion in persons without evident HIV infection — United States. MMWR Morb Mortal Wkly Rep 1992;41:541–5. - PubMed
-
- Duncan RA, von Reyn CF, Alliegro GM, Toossi Z, Sugar AM, Levitz SM. Idiopathic CD4+ T-lymphocytopenia — four patients with opportunistic infections and no evidence of HIV infection. N Engl J Med 1993;328:393–8. - PubMed
-
- Ho DD, Cao Y, Zhu T, et al. Idiopathic CD4+ T-lymphocytopenia — immunodeficiency without evidence of HIV infection. N Engl J Med 1993;328:380–5. - PubMed
-
- Spira TJ, Jones BM, Nicholson JK, et al. Idiopathic CD4+ T-lymphocytopenia — an analysis of five patients with unexplained opportunistic infections. N Engl J Med 1993;328:386–92. - PubMed
Publication types
MeSH terms
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials