

Intensivist physician-to-patient ratios and mortality in the intensive care unit
- PMID: 37133740
- PMCID: PMC10155655
- DOI: 10.1007/s00134-023-07066-z
Intensivist physician-to-patient ratios and mortality in the intensive care unit
Abstract
Purpose: A high daily census may hinder the ability of physicians to deliver quality care in the intensive care unit (ICU). We sought to determine the relationship between intensivist-to-patient ratios and mortality among ICU patients.
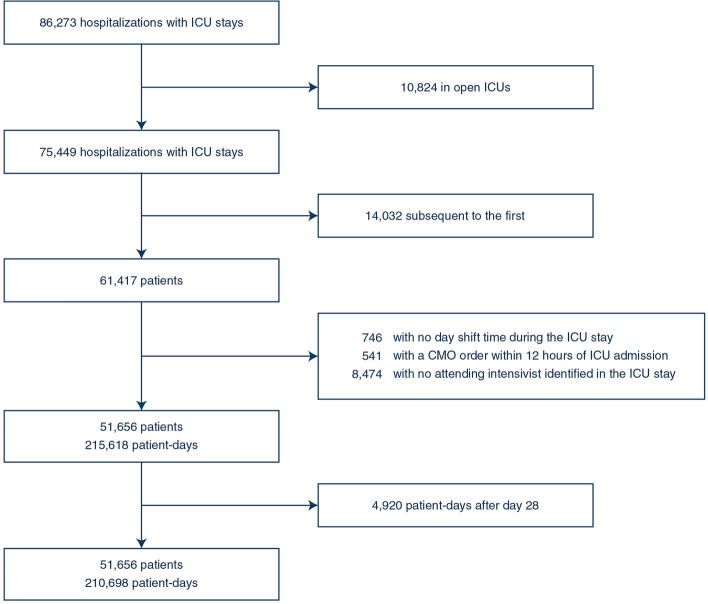
Methods: We performed a retrospective cohort study of intensivist-to-patient ratios in 29 ICUs in 10 hospitals in the United States from 2018 to 2020. We used meta-data from progress notes in the electronic health record to determine an intensivist-specific caseload for each ICU day. We then fit a multivariable proportional hazards model with time-varying covariates to estimate the relationship between the daily intensivist-to-patient ratio and ICU mortality at 28 days.
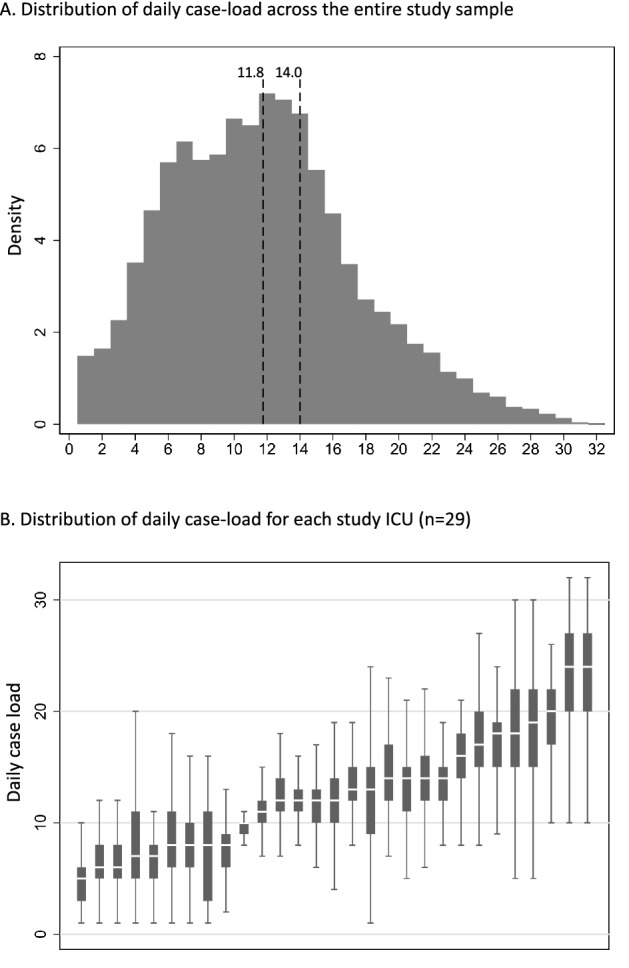
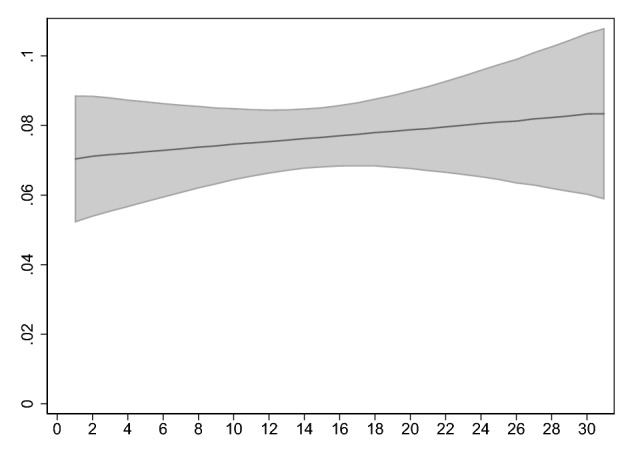
Results: The final analysis included 51,656 patients, 210,698 patient days, and 248 intensivist physicians. The average caseload per day was 11.8 (standard deviation: 5.7). There was no association between the intensivist-to-patient ratio and mortality (hazard ratio for each additional patient: 0.987, 95% confidence interval: 0.968-1.007, p = 0.2). This relationship persisted when we defined the ratio as caseload over the sample-wide average (hazard ratio: 0.907, 95% confidence interval: 0.763-1.077, p = 0.26) and cumulative days with a caseload over the sample-wide average (hazard ratio: 0.991, 95% confidence interval: 0.966-1.018, p = 0.52). The relationship was not modified by the presence of physicians-in-training, nurse practitioners, and physician assistants (p value for interaction term: 0.14).
Conclusions: Mortality for ICU patients appears resistant to high intensivist caseloads. These results may not generalize to ICUs organized differently than those in this sample, such as ICUs outside the United States.
Keywords: Critical care; Intensive care units; Physicians; Workforce; Workload.
© 2023. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors have no financial conflicts of interest to disclose.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
