

Awake prone positioning in acute hypoxaemic respiratory failure
- PMID: 37137508
- PMCID: PMC10155045
- DOI: 10.1183/16000617.0245-2022
Awake prone positioning in acute hypoxaemic respiratory failure
Abstract
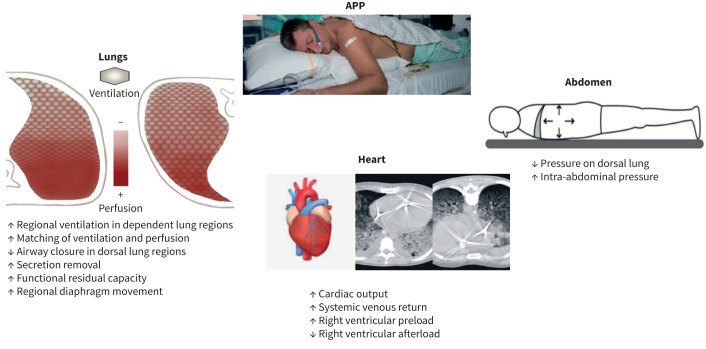
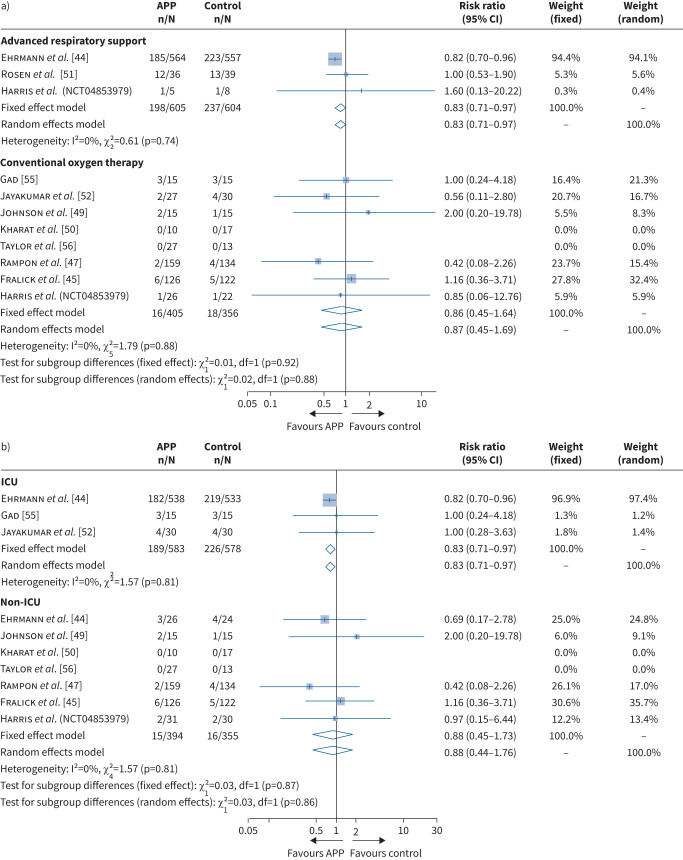
Awake prone positioning (APP) of patients with acute hypoxaemic respiratory failure gained considerable attention during the early phases of the coronavirus disease 2019 (COVID-19) pandemic. Prior to the pandemic, reports of APP were limited to case series in patients with influenza and in immunocompromised patients, with encouraging results in terms of tolerance and oxygenation improvement. Prone positioning of awake patients with acute hypoxaemic respiratory failure appears to result in many of the same physiological changes improving oxygenation seen in invasively ventilated patients with moderate-severe acute respiratory distress syndrome. A number of randomised controlled studies published on patients with varying severity of COVID-19 have reported apparently contrasting outcomes. However, there is consistent evidence that more hypoxaemic patients requiring advanced respiratory support, who are managed in higher care environments and who can be prone for several hours, benefit most from APP use. We review the physiological basis by which prone positioning results in changes in lung mechanics and gas exchange and summarise the latest evidence base for APP primarily in COVID-19. We examine the key factors that influence the success of APP, the optimal target populations for APP and the key unknowns that will shape future research.
Copyright ©The authors 2023.
Conflict of interest statement
Conflicts of interest: M. Ibarra-Estrada, A. Kharat, D. Cosgrave and C. Guerin report no conflicts of interest. B.A. McNicholas reports consulting fees received personally from Teleflex. Y. Perez reports grants to institution and personal support for attending medical congress from Fisher & Paykel. J. Li reports grants to institution from Fisher & Paykel, Aerogen, Rice Foundation and American Association for Respiratory Care; personal honoraria for lectures from Fisher & Paykel, Aerogen, Heyer lts, and American Association for Respiratory Care. I. Pavlov reports grants to institution from Open AI inc and Fisher & Paykel. D.L. Vines reports grants to institution from Teleflex Medical and Rice Foundation; personal honoraria from Theravance Biopharma; unpaid role as President, National board for Respiratory Care. O. Roca reports grants to institution from Hamilton Medical AG and Fisher & Paykel; personal consulting fees from Aerogen, and honoraria received from Hamilton Medical AG, Fisher & Paykel, Aerogen and Ambu Ltd; unpaid role as chair of Acute Respiratory Failure group of Spanish Society of Intensive Care Medicine; non-funded research support from Timpel Ltd. S. Ehrmann reports grants to institution from Aerogen Ltd and Fisher & Paykel; personal consulting fees from Aerogen Ltd; personal honoraria and support for attending meetings from Aerogen Ltd and Fisher & Paykel; participation on Data Safety Monitoring Board for Aerogen Ltd; receipt of equipment/materials from Aerogen Ltd and Fisher & Paykel. J.G. Laffey reports funding to institution from Science Foundation Ireland; personal consulting fees from Baxter Healthcare; unpaid participation in Data Safety Monitoring Board (investigator trials); unpaid role as chair of Translational Biology Section of European Society of Intensive Care Medicine.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical